

Note: All Global Research articles are now accessible in 51 languages by activating the Translate Website Drop Down Menu on the top banner of our home page.
If you want to become Member of Global Research click here
The following text is the (January 2022) updated and revised version of Chapter III of my E-Book entitled
***
“The PCR is a Process. It does not tell you that you are sick”.
Dr. Kary Mullis, Nobel Laureate and Inventor of the RT-PCR, passed away in August 2019.
“…All or a substantial part of these positives could be due to what’s called false positives tests.”
Dr. Michael Yeadon: former Vice President and Chief Science Officer for Pfizer
This misuse of the RT-PCR technique is applied as a relentless and intentional strategy by some governments to justify excessive measuressuch as the violation of a large number of constitutional rights, … under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.
.Dr. Pascal Sacré, Belgian physician specialized in critical care and renowned public health analyst.
Introduction
Media lies coupled with a systemic and carefully engineered fear campaign have sustained the image of a killer virus which is relentlessly spreading to all major regions of the World.
Several billion people in more than 190 countries have been tested (as well as retested) for Covid-19.
At the time of writing, approximately 340 million people Worldwide have been categorized as “Covid-19 confirmed cases”.
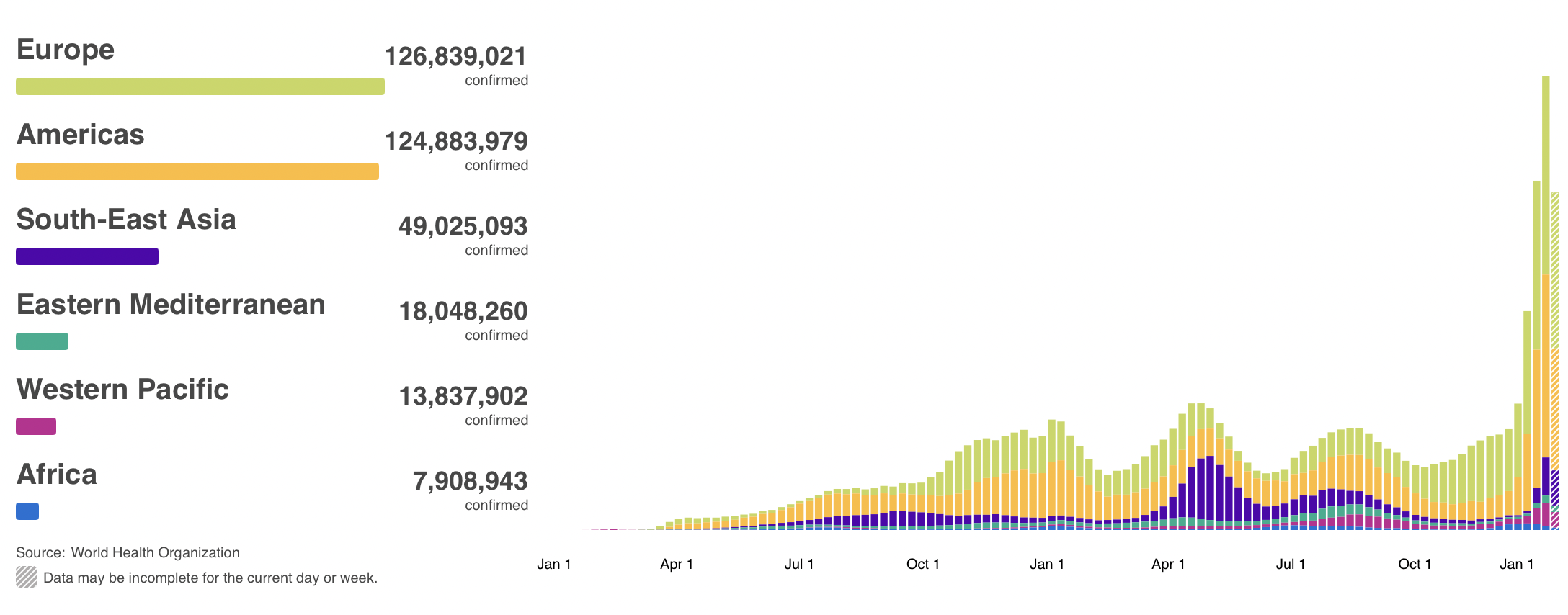
The alleged pandemic is said to have resulted in more than 5 million Covid-19 related deaths.
Both sets of figures: morbidity and mortality are invalid. A highly organized Covid testing apparatus (part of which is funded by the billionaire foundations) has been established with a view to driving up the numbers of “Covid-19 Confirmed Cases”, which are then used as a justification to impose the “vaccine” passport coupled with the repeal of fundamental human rights.
From the outset of this crisis in January 2020, all far-reaching policy decisions upheld and presented to the public as a “means to saving lives” were based on flawed and invalid RT-PCR case positives.
These invalid Covid-19 “estimates” have been used to justify confinement, social distancing, the face mask, the prohibition of social gatherings, cultural and sports events, the closure of economic activity, as well as the enforcement of the mRNA “vaccine” launched in November 2020.
There is no such thing as a “Covid-19 confirmed case”. Firmly acknowledged both by scientific opinion and the World Health Organization, the RT-PCR test used to “detect” the spread of the virus (as well as its variants) is not only flawed but TOTALLY INVALID.
The fear campaign is relentlessly spearheaded by political statements and media disinformation. A closer examination of official reports from national health authorities as well as peer reviewed articles provides a totally different picture.
In this chapter we will be focussing on the following issues:
1. The features of the SARS-CoV-2 virus as outlined by the WHO, the CDC and peer reviewed reports. Is it a dangerous virus?
2. The Reverse Transcription Polymerase Chain Reaction Test (RT-PCR) used to “detect / identify” SARS-CoV-2
3. the reliability of the estimates of mortality and morbidity pertaining to the alleged Covid-19 infection.
The Features of SARS-CoV-2
Lies through omission: the media has failed to reassure the broader public.
Below is the official WHO definition of Covid-19 followed by that of the CDC:
Coronaviruses are a large family of viruses which may cause illness in animals or humans. In humans, several coronaviruses are known to cause respiratory infections ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS). The most recently discovered coronavirus causes coronavirus disease COVID-19.
“The most common symptoms of COVID-19 are fever, dry cough, and tiredness. … These symptoms are usually mild and begin gradually. Some people become infected but only have very mild symptoms. Most people (about 80%) recover from the disease without needing hospital treatment. Around 1 out of every 5 people who gets COVID-19 becomes seriously ill and develops difficulty breathing.”

Screenshot The Hill, March 19, 2020
Similar to Influenza according to the CDC
Covid-19 versus Influenza (Flu) Virus A and Virus B (and subtypes)
Rarely mentioned by the media or by politicians: The CDC (which is an agency of the US government) confirms that Covid-19 is similar to Influenza
“Influenza (Flu) and COVID-19 are both contagious respiratory illnesses, but they are caused by different viruses. COVID-19 is caused by infection with a new coronavirus (called SARS-CoV-2) and flu is caused by infection with influenza viruses. Because some of the symptoms of flu and COVID-19 are similar, it may be hard to tell the difference between them based on symptoms alone, and testing may be needed to help confirm a diagnosis. Flu and COVID-19 share many characteristics, but there are some key differences between the two.”
If the public had been informed and reassured that Covid is “similar to Influenza”, the fear campaign would have fallen flat.
The lockdown and closure of the national economy would have been rejected outright.
According to Dr. Wolfgang Wodarg, pneumonia is “regularly caused or accompanied by corona viruses”.
Immunologists broadly confirm the CDC definition. COVID-19 has similar features to a seasonal influenza coupled with pneumonia.
According to Anthony Fauci (Head of NIAID), H. Clifford Lane and Robert R. Redfield (Head of CDC) in the New England Journal of Medicine
“…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
Dr. Anthony Fauci is lying to himself. In his public statements he says that Covid is “Ten Times Worse than Seasonal Flu”.
He refutes his peer reviewed report quoted above. From the outset, Fauci has been instrumental in waging a fear and panic campaign across America:

Screenshot The Hill, March 19, 2020
The Reverse Transcription Polymerase Chain Reaction Test (RT-PCR)
The slanted methodology applied under WHO guidance for detecting the alleged spread of the virus is the Polymerase Chain Reaction Test (RT-PCR), which has been routinely applied all over the World since February 2020.
The RT-PCR Test has been used Worldwide to generate millions of erroneous “Covid-19 Confirmed Cases”, which are then used to sustain the illusion that the alleged pandemic is Real.
This assessment based on erroneous numbers has been used in the course of the last two years to spearhead and sustain the fear campaign.
And people are now led to believe that the Covid-19 “vaccine” is the “solution”. And that “normality” will be restored once the entire population of Planet Earth has been vaccinated.
“Confirmed” is a misnomer: A “Confirmed RT-PCR Positive Case” does not imply a “Covid-19 Confirmed Case”.
Positive RT-PCR is not synonymous with the COVID-19 disease! PCR specialists make it clear that a test must always be compared with the clinical record of the patient being tested, with the patient’s state of health to confirm its value [reliability] (Dr. Pascal Sacré)
The procedure used by the national health authorities is to categorize all RT-PCR positive cases, as “Covid-19 Confirmed Cases” (with or without a medical diagnosis). Ironically, this routine process of identifying “confirmed cases” . is in derogation of the CDC’s own guidelines:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms. The performance of this test has not been established for monitoring treatment of 2019-nCoV infection. This test cannot rule out diseases caused by other bacterial or viral pathogens.” (emphasis added)
The methodology used to detect and estimate the spread of the virus is flawed and invalid.
False Positives
The earlier debate at the outset of the crisis focused on the issue of “False Positives”.
Acknowledged by the WHO and the CDC, the RT-PCR Test was known to produce a high percentage of false positives. According to Dr. Pascal Sacré:
“Today, as authorities test more people, there are bound to be more positive RT-PCR tests. This does not mean that COVID-19 is coming back, or that the epidemic is moving in waves. There are more people being tested, that’s all.”
The debate on false positives (acknowledged by the health authorities) points to so-called errors without necessarily questioning the overall validity of the RT-PCR test as a means to detecting the alleged spread of the CoV-SARS-2 virus.
The PCR-Test Does Not Detect the Identity of the Virus
The RT-PCR test does not identify/ detect the virus. What the PCR test identifies are genetic fragments of numerous viruses (including influenza viruses types A and B, and coronaviruses which trigger common colds).
The results of the RT-PCR test cannot “confirm” whether an individual who undertakes the test is infected with SARS-CoV-2.
The following diagram summarizes the process of identifying positive and negative cases: All that is required is the presence of “viral genetic material” for it to be categorized as “positive”. The procedure does not identity or isolate Covid-19. What appears in the tests are fragments of the virus.
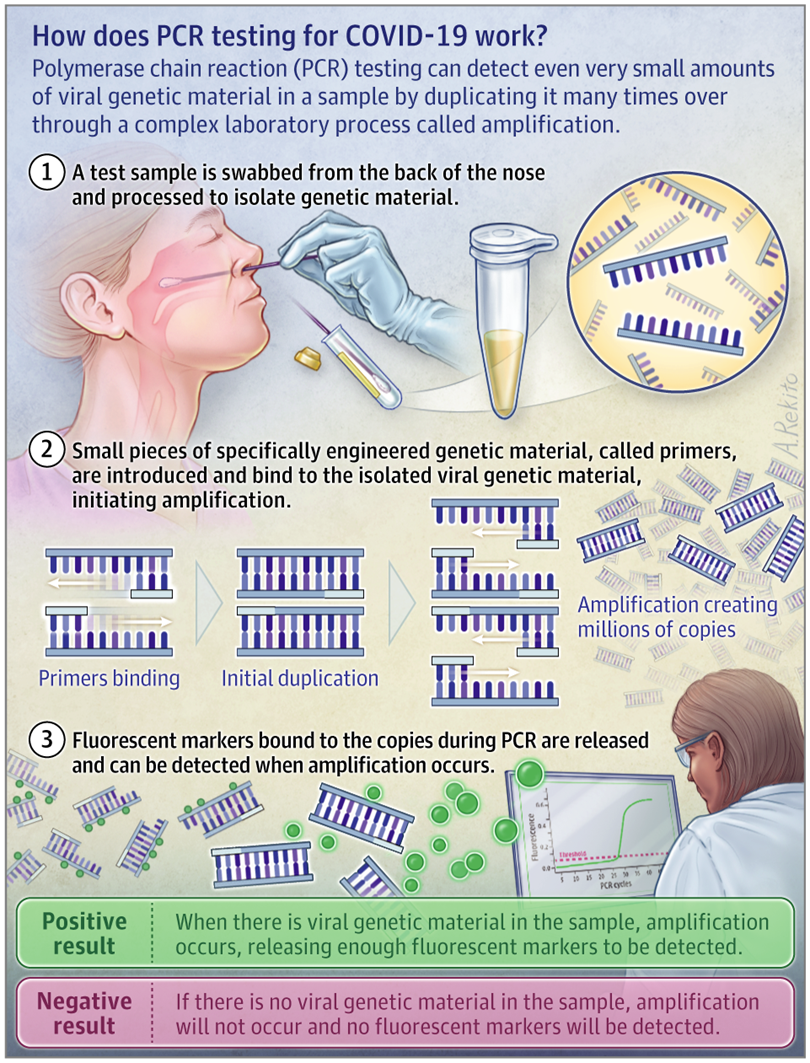
According to Dr. Kary Mullis, inventor of the PCR technique: “The PCR detects a very small segment of the nucleic acid which is part of a virus itself.”
According to renowned Swiss immunologist Dr B. Stadler
So if we do a PCR corona test on an immune person, it is not a virus that is detected, but a small shattered part of the viral genome. The test comes back positive for as long as there are tiny shattered parts of the virus left. Even if the infectious viri are long dead, a corona test can come back positive, because the PCR method multiplies even a tiny fraction of the viral genetic material enough [to be detected].
Dr. Pascal Sacré concurs: “These tests detect viral particles, genetic sequences, not the whole virus.”
In an attempt to quantify the viral load, these sequences are then amplified several times through numerous complex steps that are subject to errors, sterility errors and contamination.”
The WHO’s “Customized” RT-PCR Covid-19 “Test”
Two important and related issues.
The PCR Test does not identify the virus as outlined above. Moreover, the WHO in January 2020, did not possess an isolate and purified sample of the novel 2019-nCov virus.
What was contemplated in January 2020 was a “customization”of the PCR test by the WHO, under the scientific guidance of the Berlin Virology Institute at Charité Hospital.
Dr. Christian Drosten, and his colleagues of the Berlin Virology Institute undertook a study entitled, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR”.
The title of the Berlin Virology Institute Study is an obvious misnomer. The PCR test cannot “detect” the 2019 novel coronavirus. (See Dr. Kary Mullis, Dr. B. Stadler, Dr. Pascal Sacré quoted above).
Moreover, the study, published by Eurosurveillance acknowledges that the WHO did not possess an isolate and purified sample of the novel 2019-nCov virus:
[While]… several viral genome sequences had been released,… virus isolates or samples [of 2019-nCoV] from infected patients were not available …”
The Drosten et al team then recommended to the WHO, that in the absence of an isolate of the 2019-nCoV virus, a similar 2003-SARS-CoV should be used as a “proxy” (point of reference) of the novel virus:
“The genome sequences suggest presence of a virus closely related to the members of a viral species termed severe acute respiratory syndrome (SARS)-related CoV, a species defined by the agent of the 2002/03 outbreak of SARS in humans [3,4].
We report on the the establishment and validation of a diagnostic workflow for 2019-nCoV screening and specific confirmation [using the RT-PCR test], designed in absence of available virus isolates or original patient specimens. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.” (Eurosurveillance, January 23, 2020, emphasis added).
What this ambiguous statement suggests is that the identity of 2019-nCoV was not required and that “Covid-19 Confirmed Cases” (aka infection resulting from the novel 2019 coronavirus) would be validated by “the close genetic relatedness to the 2003-SARS-CoV.”
What this means is that a coronavirus detected 19 years ago (2003-SARS-CoV) is being used to “validate” the identity of a so-called “novel coronavirus” first detected in China’s Hubei Province in late December 2019.
The recommendations of the Drosten study (generously supported and financed by the Gates Foundation) were then transmitted to the WHO. They were subsequently endorsed by the Director General of the WHO, Dr. Tedros Adhanom.
The WHO did not have in its possession the “virus isolate” required to identify the virus. It was decided that an isolate of the new coronavirus was not required.
The Drosten et al article pertaining to the use of the RT-PCR test Worldwide (under WHO guidance) was challenged in a November 27, 2020 study by a group of 23 international virologists, microbiologists et al.
It stands to reason that if the PCR test uses the 2003 SARS- CoV virus as “a point of reference”, there can be no “confirmed” Covid-19 cases of the novel virus 2019-nCoV (subsequently renamed SARS-CoV-2) or of its variants.
Has the Identity of the 2019-nCoV Been Confirmed? Does the Virus Exist?
While the WHO did not possess an isolate of the virus, is there valid and reliable evidence that the 2019 novel coronavirus had been isolated from an “unadulterated sample taken from a diseased patient”?
The Chinese authorities announced on January 7, 2020 that “a new type of virus” had been “identified” “similar to the one associated with SARS and MERS” (related report, not original Chinese government source). The underlying method adopted by the Chinese research team is described below:
We prospectively collected and analysed data on patients with laboratory-confirmed 2019-nCoV infection by real-time RT-PCR and next-generation sequencing.
Data were obtained with standardised data collection forms shared by WHO and the International Severe Acute Respiratory and Emerging Infection Consortium from electronic medical records. (emphasis added)
The above study (quotation above as well as other documents consulted ) suggest that China’s health authorities did not undertake an isolation / purification of a patient’s specimen. Using “laboratory-confirmed 2019-nCoV infection by real-time RT-PCR” (as quoted in their study) is an obvious misnomer, i.e. the RT-PCR test cannot under any circumstances be used to identify the virus. The isolate of the virus by the Chinese authorities is unconfirmed.
Freedom of Information Pertaining to the Isolate of SARS-CoV-2
A detailed investigative project by Christine Massey, entitled: Freedom of Information Requests: Health/ Science Institutions Worldwide “Have No Record” of SARS-COV-2 Isolation/Purification provides documentation concerning the identity of the virus. The responses to these requests from 127 entities in 25 countries confirm that there is no record of isolation / purification of SARS-CoV-2 “having been performed by anyone, anywhere, ever.”
The Threshold Amplification Cycles. The WHO Admits that The Results of the RT-PCR “Test” are Totally Invalid
The rRT-PCR test was adopted by the WHO on January 23, 2020 as a means to detecting the SARS-COV-2 virus, following the recommendations of the Berlin Virology research group (quoted above).
Exactly one year later on January 20th, 2021, the WHO retracts. They don’t say “We Made a Mistake”. The retraction is carefully formulated. (See original WHO document here)
The contentious issue pertains to the number of amplification threshold cycles (Ct). According to Pieter Borger, et al
The number of amplification cycles [should be] less than 35; preferably 25-30 cycles. In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture…(Critique of Drosten Study)
The World Health Organization (WHO) tacitly admits one year later that ALL PCR tests conducted at a 35 cycle amplification threshold (Ct) or higher are INVALID. But that is what they recommended in January 2020, in consultation with the virology team at Charité Hospital in Berlin.
If the test is conducted at a 35 Ct threshold or above (which was recommended by the WHO), genetic segments of the SARS-CoV-2 virus cannot be detected, which means that ALL the so-called “Covid-19 Confirmed Cases” tabulated Worldwide in the course of the last two years are invalid.
According to Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, et al, the Ct > 35 has been the norm “in most laboratories in Europe & the US”.
The WHO’s Mea Culpa
Below is the WHO’s carefully formulated “Retraction”.
“WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology. (emphasis added)
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.”
“Invalid Positives” is the Underlying Concept
This is not an issue of “Weak Positives” and “Risk of False Positive Increases”. What is at stake is a “Flawed Methodology” which leads to invalid estimates of “Confirmed Covid-19 Cases”.
What this admission of the WHO confirms is that the estimate of covid positive from a PCR test (with an amplification threshold of 35 cycles or higher) is invalid. In which case, the WHO recommends retesting: “a new specimen should be taken and retested…”.
The WHO calls for “Retesting”, which is tantamount to saying “We Screwed Up”.
That recommendation is pro-forma. It won’t happen. Several billion people Worldwide have already been tested, starting in early February 2020.
From the outset, the PCR test has routinely been applied at a Ct amplification threshold of 35 cycles or higher. What this means is that the PCR methodology as applied Worldwide has in the course of the last two years led to the compilation of faulty and misleading Covid-19 estimates, which according to the WHO (January 20, 2021) are based on an invalid methodology.
And these are the statistics which are used to measure the progression of the so-called “pandemic”. Above an amplification cycle of 35 or higher, the test will not detect fragments of the virus. Therefore, the official “covid numbers” ( Covid-19 Confirmed Cases) are meaningless.
It follows that there is no scientific basis for confirming the existence of a pandemic.
Which in turn means that the lockdown / economic measures which have resulted in social panic, mass poverty and unemployment (allegedly to curtail the spread of the virus) have no justification whatsoever. According to scientific opinion:
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97% (Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, Clare Craig, Kevin McKernan, et al, Critique of Drosten Study)
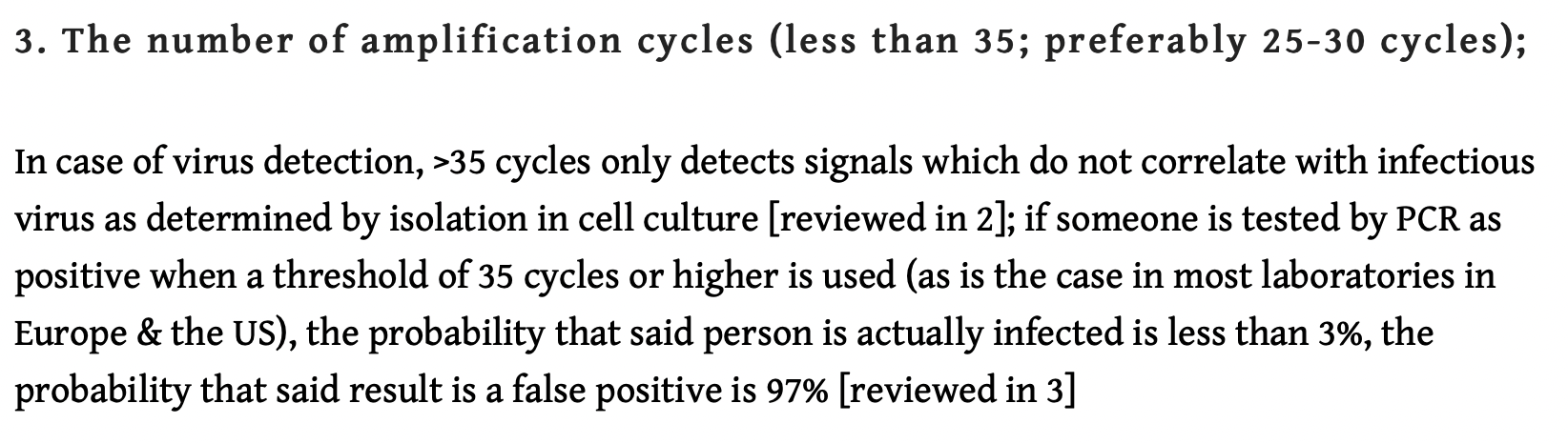
As outlined above, “the probability that said result is a false positive is 97%”: It follows that using the >35 cycles detection will indelibly contribute to “hiking up” the number of “fake positives”.
The WHO’ Mea Culpa confirms that the Covid-19 PCR test procedure as applied is meaningless.
The CDC Orders the Withdrawal of the PCR Test
The WHO’s historic retraction is followed six months later by a Mea Culpa on the part of the CDC. On July 21, 2021, the Centers for Disease Control and Prevention (CDC) calls for the withdrawal of the PCR test as a valid method for detecting and identifying SARS-CoV-2:
“After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only.”
In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test.
CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. (emphasis added)
Read carefully, what this CDC directive tacitly admits is that the PCR test does not effectively differentiate between “SARS-CoV-2 and influenza viruses”. We have known this from the outset.
As of January 1, 2022, the CDC has withdrawn it’s endorsement of the RT-PCR test in the U.S.
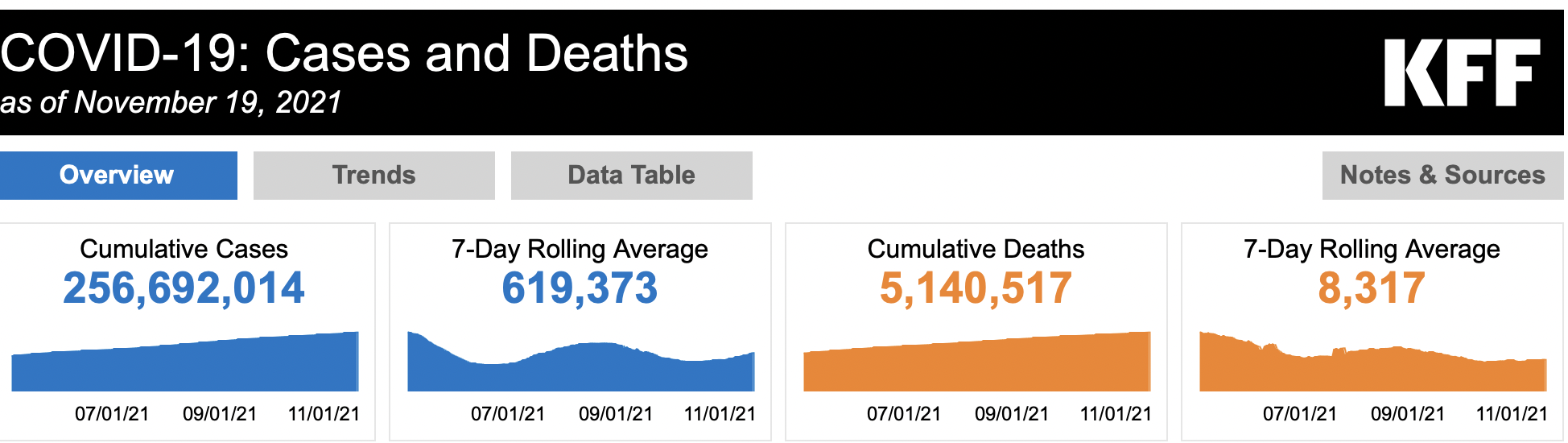
If the PCR test is invalid as intimated both by the CDC and the WHO, more than 260 Million so-called “Covid-19 Confirmed Cases” as well as more than 5 million Covid related deaths collected and tabulated Worldwide since the outset of the alleged pandemic are totally meaningless.
The Falsification of Death Certificates
Inasmuch as the PCR test is invalid, it follows that the estimates of “Covid-19 Confirmed Cases” including the detection of variants of SARS-CoV-2 are totally invalid. This in turn means that the methodology pertaining to establishing Covid-19 related deaths Worldwide is also invalid.
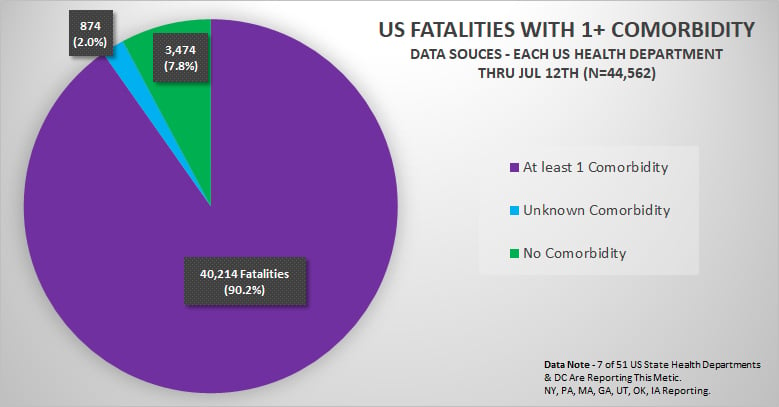
It is worth noting that in a December 2020 report, the CDC reported that 94% of the deaths attributed to Covid have “comorbidities”,(i.e. deaths dues other causes).
For 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death. The number of deaths with each condition or cause is shown for all deaths and by age groups.
Moreover, had the CDC used the criteria in its Medical Examiners’ and Coroners’ Handbook on Death Registration and Fetal Death Reporting Revision 2003:
” … the COVID-19 fatality count would have been approximately 90.2% lower” (See , August 09, 2020)
COVID-19: The “Underlying Cause of Death” and the CDC’s “More Often Than Not” Clause
While the CDC acknowledged the issue of comorbidities, it nonetheless enacted totally invalid instructions with regard to the Death Certificates.
Barely a week following the historic March 11, 2020 lockdown, specific guidelines were introduced by the CDC pertaining to Death Certificates (and their tabulation in the National Vital Statistics System (NVSS).
The underlying cause of death is defined by the WHO as
“the disease or injury that initiated the train of events leading directly to death”.
What the CDC recommended with regards to statistical coding and categorization is that COVID-19 is expected to be the underlying cause of death“more often than not.”
The CDC combines these two criteria. “underlying cause of death”, “more often than not”.
Will COVID-19 be the underlying cause of death?
“The underlying cause depends upon what and where conditions are reported on the death certificate. However, the rules for coding and selection of the underlying cause of death are expected to result in COVID- 19 being the underlying cause more often than not.”
The above directive is categorical.
The CDC concepts and justifications
The Certifier is not allowed to report coronavirus without identifying a specific strain. And the guidelines recommend that COVID-19 must always be indicated.
The certifier cannot depart from the CDC criteria. Covid-19 is imposed. Read carefully the CDC criteria):
There are no loopholes. These CDC directives have contributed to categorizing Covid-19 as the recorded “cause of death”. Two fundamental concepts prevail throughout:
- The “underlying cause of death”
- The “More Often than Not” Clause which falsifies the Cause of Death
And these criteria are imposed despite the fact that the RT-PCR test used to corroborate the “cause of death” provides misleading results as acknowledged by both the WHO and the CDC.
In practice, as outlined above: “probable COVID-19” or “likely COVID-19,” will be considered as the “underlying cause of death” without the conduct of a PCR test and without performing an autopsy.
The criteria establishing the “underlying” Cause of Death in the US are based on “the more often than not” clause (see above) established nationally by the CDC.
Canada: Flawed “Estimates” of the Cause of Death
In Canada, the criteria differ from one province to another. Categorizing the cause of death in Canada’s Province of Quebec has been the object of gross manipulation.
According to a directive from Quebec’s Ministry of Health (April 2020):
“If the presumed cause of death is Covid-19 (with or without a positive test) an autopsy should be avoided and death should be attributed to Covid-19 as the probable cause of death. In addition, deaths whose probable cause is Covid-19 are considered natural, and are not subject to a coroner’s notice. “ (emphasis in the original document).
The directive does not allow the counting of co-morbidities. Applied on April 16, 2020, this directive was conducive to an immediate sharp increase in the number of deaths attributed to Covid-19:
44.9% of total deaths in Quebec were attributed to Covid-19 (week of 11-18 April 2020) (see table below).
According to Montreal’s La Presse, “April [2020] was the deadliest month” . But did La Presse consult the directives of the Ministry of Health?
Below are the (daily) causes of death for Quebec corresponding to the week of April 12 to 18, 2020 (immediately following the government directive) measured according to the criteria issued by the Ministry of Health.

Are these figures the result of the so-called deadly pandemic? Or are they the result of the Ministry of Health’s “guidelines” based on erroneous criteria?
- “presumed” case pertaining to Covid,
- “With or without a positive test”,
- “probable” cause of death,
- “Autopsy should be avoided” in the case of Covid-19.
- “ Deaths of which the probable cause is Covid-19, are considered natural, and are not the object of a notice to the coroner “
According to Mr. Paul G. Brunet, of the Council for the protection of the sick (CPM):
“… We realized through the denunciations by some of the doctors that people did not die from COVID, but from dehydration, malnutrition, abandonment, laments Mr. Brunet. So what did the thousands of people in CHSLDs [old persons nursing homes] and private residences really die of?” (quoted in La Presse, translated from French)
Test, Test, Test: Invalid Data and the “Numbers’ Game”
People are frightened. They are encouraged to do the PCR test, which increases the number of fake positives. Governments are involved in increasing the number of PCR tests with a view to inflating the estimates of so-called “Covid-19 confirmed cases”.
In 2021-2022, the new antigen rapid test (which can be done at home) is being adopted in a large number of countries.
In Canada which has a population of 38.5 million people, the federal government has ordered the delivery of 234 million Covid-19 antigen home testing kits. This decision has not only contributed to spearheading the fear campaign, it has created a situation of social chaos. Moreover, these tests are not routinely accompanied by a medical diagnosis of the patients.
Annex to Chapter III
Full text of the WHO directive dated January 20, 2021
Nucleic Acid Testing (NAT) Technologies that Use Polymerase Chain Reaction (PCR) for Detection of SARS-CoV-2
Product type: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2
Date: 13 January 2021
WHO-identifier: 2020/5, version 2
Target audience: laboratory professionals and users of IVDs.
Purpose of this notice: clarify information previously provided by WHO. This notice supersedes WHO Information Notice for In Vitro Diagnostic Medical Device (IVD) Users 2020/05 version 1, issued 14 December 2020.
Description of the problem: WHO requests users to follow the instructions for use (IFU) when interpreting results for specimens tested using PCR methodology.
Users of IVDs must read and follow the IFU carefully to determine if manual adjustment of the PCR positivity threshold is recommended by the manufacturer.
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information.
Actions to be taken by IVD users:
- Please read carefully the IFU in its entirety.
- Contact your local representative if there is any aspect of the IFU that is unclear to you.
- Check the IFU for each incoming consignment to detect any changes to the IFU.
- Provide the Ct value in the report to the requesting health care provider.
Notes
1. Diagnostic testing for SARS-CoV-2. Geneva: World Health Organization; 2020, WHO reference number WHO/2019-nCoV/laboratory/2020.6.
2. Altman DG, Bland JM. Diagnostic tests 2: Predictive values. BMJ. 1994 Jul 9;309(6947):102. doi: 10.1136/bmj.309.6947.102.