


All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
***
I recently had a parent write to me that the overnight camp that they were going to send their child to (fees already paid), had just notified them that mask use was to be required of students at all times. Was there anything I could do? Unfortunately, I can not change the mind-set of a summer camp on the west coast. The CDC is once again promoting policies with no basis in scientific fact, but these policies are reflexively accepted by those whom we trust to care for our children.
COVID may be “over” for many of us, but not so for many of our children.
*
Environ Res. 2022 Sep; 212: 113564. 2022 May 28. doi: 10.1016/j.envres.2022.113564
This shocking paper had no coverage by the state-sponsored media, even though it shows that the average CO2 levels in inhaled air with nose and mouth coverings in children between age 6 and 17 is well beyond acceptable levels.
From the Abstract
We used short term measurements under surgical masks and FFP2 masks according to European norm EN 149, compared to baseline in an experimental, intra-individually controlled study over 25 min. CO2 content was measured every 15 s using an automated dual-wavelength infrared CO2 measurement device (G100, Geotech, Leamington Spa, UK) over 25 min in a short-term experimental setting, with children seated. After baseline measurement children were provided with two types of commonly worn NMC: surgical masks and FFP2–masks in randomized sequence for 3 min each. We kept ambient CO2-levels below 1000 parts per million (ppm) through frequent ventilation. We measured breathing frequency and pulse as potential physiological moderator variables. Forty-five children, 25 boys, 20 girls, with a mean age of 10.7 years (standard deviation 2.6) were measured. We measured 13,100 ppm (SD 380) under surgical mask and 13,900 ppm (SD 370) under FFP2 mask in inhaled air. A linear model with age as a covariate showed a highly significant effect of the condition (p < 1*10−9). We measured 2,700 ppm (SD 100) CO2 at pre-baseline and 2,800 ppm (SD 100) at post-baseline, a non-significant small difference. Appropriate contrasts revealed that the change was due to the masks only and the difference between the two types of masks was small and not significant. Wearing of NMC (surgical masks or FFP2- -masks) raises CO2 content in inhaled air quickly to a very high level in healthy children in a seated resting position that might be hazardous to children’s health.
From the Conclusions:
In conclusion we have produced experimental data that show that carbon dioxide content in inhaled air rises on average to 13,000 to 13,750 ppm no matter whether children wear a surgical or an FFP2 mask. This is far beyond the level of 2,000 ppm considered the limit of acceptability and beyond the 1,000 ppm that are normal for air in closed rooms. This estimate is rather on the low side, as we only measured this after a short time without physical exertion. Decision makers and law courts should take this into consideration when establishing rules and guidance to fight infections.
*
Another recent study showing another major issue with masking:
Face masks disrupt holistic processing and face perception in school-age children
Cogn Res Princ Implic. 2022 Feb 7. doi: 10.1186/s41235-022-00360-2
This paper’s conclusion:
The current study provides evidence for quantitative and qualitative changes in the processing of masked faces in children. Changes in face recognition performance and alteration in the processing of partially occluded faces could have significant effects on children’s social interactions with their peers and their ability to form relationships with educators. Previous research in adults has already demonstrated the detrimental effect of reduced face perception abilities on one’s level of social confidence and quality of life
*
For the full and complete resource on the dangers of masking, the Brownstone Institute has documented over 150 comparative studies and articles on mask ineffectiveness and harms.
Brownstone Institute, DECEMBER 20, 2021
Sadly, our children will bear the catastrophic consequences and not just educationally, of the deeply flawed school closure policy for decades to come (particularly our minority children who were least able to afford this). Many are still pressured to wear masks and punished for not doing so.
The annotated bibliography in this article is very compelling and shows that masking has significant harms. These studies are clear that masks do not work to control the virus and that masking can be harmful, particularly to children.
*
However, The CDC still recommends masking of K-12 students if the community levels of COVID are high or if there are students in the school who might get very sick from COVID.
From the CDC website:
“ECE (Early Childhood Education) programs may choose to implement universal indoor mask use to meet the needs of the families they serve, which could include people at risk for getting very sick with COVID-19.”
“Schools with students at risk for getting very sick with COVID-19 must make reasonable modifications when necessary to ensure that all students, including those with disabilities, are able to access in-person learning. Schools might need to require masking, based on federal, state, or local laws and policies, to ensure that students with immunocompromising conditions or other conditions that increase their risk for getting very sick with COVID-19 can access in-person learning.”
The CDC lists 20% of the USA as being at “high risk” for COVID.
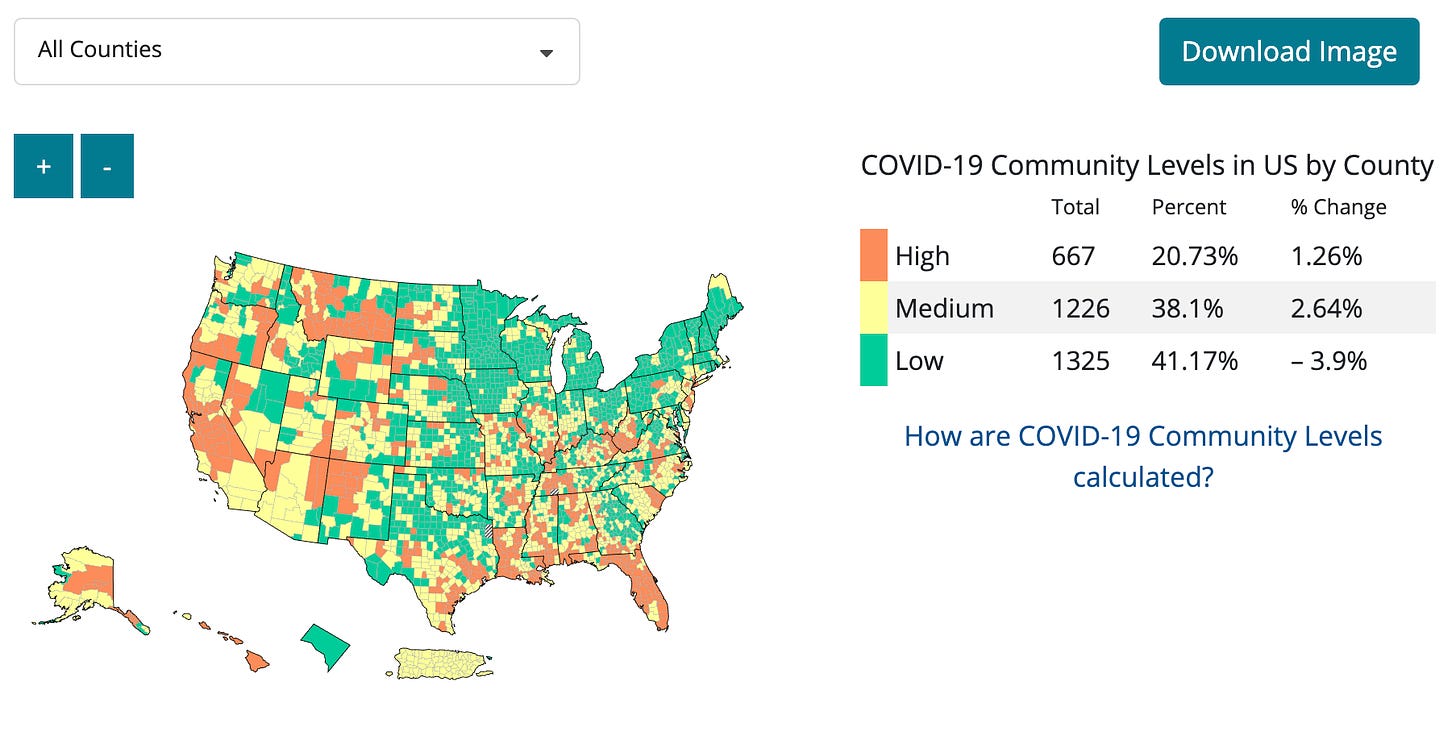
So, what do they recommend for areas that they place in the “high COVID-19 Community levels”
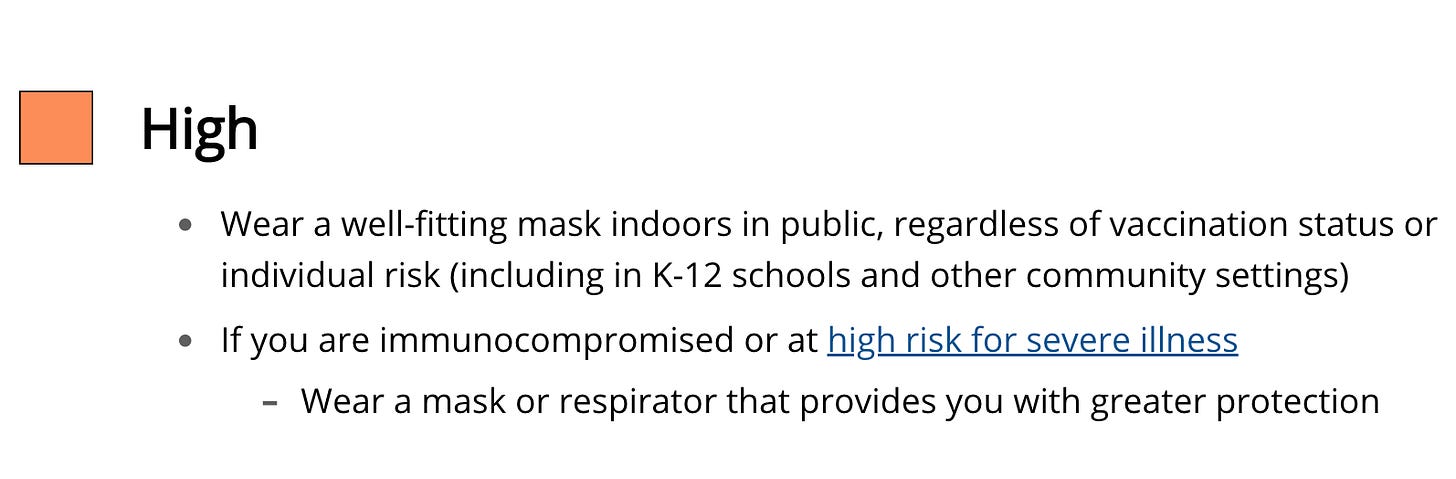
Yep- basically the CDC still recommends masks for over 20% of our K-12 children. They also recommend that ALL children be masked if there are children who might become very sick in the classroom. That children at risk for sever COVID must not be separated in any way, but instead the entire school should be masked to protect the vulnerable… this includes those children in early education programs.
*
Josh Stevenson, in an April 21, 2022 Brownstone Institute article entitled “The Mask Studies You Should Know” has summarized many of the key papers:
“There was no reduction in per-population daily mortality, hospital bed, ICU bed, or ventilator occupancy of COVID-19-positive patients attributable to the implementation of a mask-wearing mandate”
Use of face masks did not impact COVID-19 incidence among 10–12-year-olds in Finland
“We compared the differences in trends of 14-day incidences between Helsinki and Turku among 10–12-year-olds, and for comparison, also among ages 7–9 and 30–49 by using join point regression. According to our analysis, no additional effect seemed to be gained from this, based on comparisons between the cities and between the age groups of the unvaccinated children (10–12 years versus 7–9 years)”
Mask mandate and use efficacy in state-level COVID-19 containment
“Mask mandates and use are not associated with slower state-level COVID-19 spread during COVID-19 growth surges”
CEREBRAL CORTEX: Reading Covered Faces
“ Au fait research on reading covered faces reveals that: 1) wearing masks hampers facial affect recognition, though it leaves reliable inferring basic emotional expressions; 2) by buffering facial affect, masks lead to narrowing of emotional spectrum and dampen veridical evaluation of counterparts; 3) masks may affect perceived face attractiveness; 4) covered (either by masks or other veils) faces have a certain signal function introducing perceptual biases and prejudices; 5) reading covered faces is gender- and age-specific, being more challenging for males and more variable even in healthy aging; 6) the hampering effects of masks on social cognition occur over the globe; and 7) reading covered faces is likely to be supported by the large-scale assemblies of the neural circuits far beyond the social brain.”
Masking Emotions: Face Masks Impair How We Read Emotions
“The main insight of the present research is that face masks’ use influences emotion inference from faces for all ages and especially for toddlers.”
Making pre-school children wear masks is bad public health
“In summary, the benefits of masking pre-school children are unclear but are probably too small to make a major difference to individuals risks from SARS-CoV-2 or epidemic control (even before considering variable likely compliance amongst toddlers). In contrast, the harms of this policy are likely to be damaging, potentially considerably so. Given this, and the influence that the CDC and Dr Fauci have both in the US and globally, we believe an urgent re-consideration of this policy is needed”
Little evidence for facemask use in children against COVID-19
“Face masks also have potential disadvantages, such as hindering verbal and non-verbal communication. There is a risk that children will keep touching their masks and actually increase the viral load on their hands. Using face masks also risks replacing social distancing, as some parents may be tempted to send their children to school or daycare wearing a mask if they have minor symptoms rather than keeping them at home. Finally, the commercially made masks that are currently available, especially the N95 masks that are said to offer greater protection, rarely fit children. Hence the use of such masks might lead to a false sense of safety, despite leaking viruses due to their poor fit. However, the most important drawback of face masks in children may well be that their use could reduce the focus from other measures that may be more important, such as hand washing, social distancing and staying at home when they are sick.”
Wearing N95, Surgical, and Cloth Face Masks Compromises the Perception of Emotion
“Across conditions, participants perceived significantly lower levels of the expressed (target) emotion in masked faces, and this was particularly true for expressions composed of more facial action in the lower part of the face. Higher levels of other (non-target) emotions were also perceived in masked expressions. In the second study, participants rated the extent to which three categories of smiles (reward, affiliation, and dominance) conveyed positive feelings, reassurance, and superiority, respectively. Masked smiles communicated less of the target signal than unmasked smiles, but not more of other possible signals. The present work extends recent studies of the effects of masked faces on the perception of emotion in its novel use of dynamic facial expressions (as opposed to still images) and the investigation of different types of smiles.”
Face Masks Impair Basic Emotion Recognition
“These main effects indicated that emotion recognition was significantly reduced overall when faces wore masks (M = 0.52, SE = 0.007) relative to when they did not (M = 0.75, SE = 0.007) with this reduction evident across all emotions”
“Results showed that the ability to identify all facial expressions decreased when faces were masked, a finding observed across all three studies, contradicting previous research on fear, sad, and neutral expressions. Participants were also less confident in their judgements for all emotions, supporting previous research; and participants perceived emotions as less expressive in the mask condition compared to the unmasked condition, a finding novel to the literature. An additional novel finding was that participants with higher scores on the AQ-10 were less accurate and less confident overall in facial expression recognition, as well as perceiving expressions as less intense. Our findings reveal that wearing face masks decreases facial expression recognition, confidence in expression identification, as well as the perception of intensity for all expressions, affecting high-scoring AQ-10 individuals more than low-scoring individuals.”
“Standard surgical and custom apron shield masks significantly hampered word recognition, even in quiet conditions.”
Face masks reduce emotion-recognition accuracy and perceived closeness
“Our preregistered study with 191 German adults revealed that face masks diminish people’s ability to accurately categorize an emotion expression and make target persons appear less close. Exploratory analyses further revealed that face masks buffered the negative effect of negative (vs. non-negative) emotion expressions on perceptions of trustworthiness, likability, and closeness.”
“High rates of fungal contamination observed in our study emphasizes the need for better mask hygiene in the COVID-19 era”
Short report on the effects of SARS-CoV-2 face protective equipment on verbal communication
“The use of face personal protective equipment causes significant verbal communication issues. Healthcare workers, school-aged children, and people affected by voice and hearing disorders may represent specific at-risk groups for impaired speech intelligibility.”
“However, the warning of Palmeiri et al.5 for the possible future consequences caused by a poorly regulated use of nanotechnology in textiles should be extended to face masks where TiO2 particles are applied conventionally, as a white colorant or as a matting agent, or to assure durability reducing polymer breakdown by ultraviolet light3,4. These properties are not critical for the functioning of face masks, and synthetic fibers suitable for face mask can be produced without TiO229 as was observed in the layers of several masks (Table 1). Moreover, uncertainties regarding the genotoxicity of TiO2 particles remain14. Therefore, these results urge for the implementation of regulatory standards phasing out or limiting the amount of TiO2 particles, according to the ‘safe-by-design’ principle.”
“the risk of inhaling plastic microfibers, particles, and fragments from the inside of masks and respirators has only been anecdotally examined”
“This study including 19504 blood donors spanning over one and a half year shows that prolonged use of face mask by blood donors may lead to intermittent hypoxia and consequent increase in hemoglobin mass”
*
But it gets worse…
Headstart, which enrolls babies, toddlers and young children still requires universal masking –if the child is aged of two years old or older. Headstart serves over a million children per year – and most of these must be masked. Yep, you read that right. From their website:
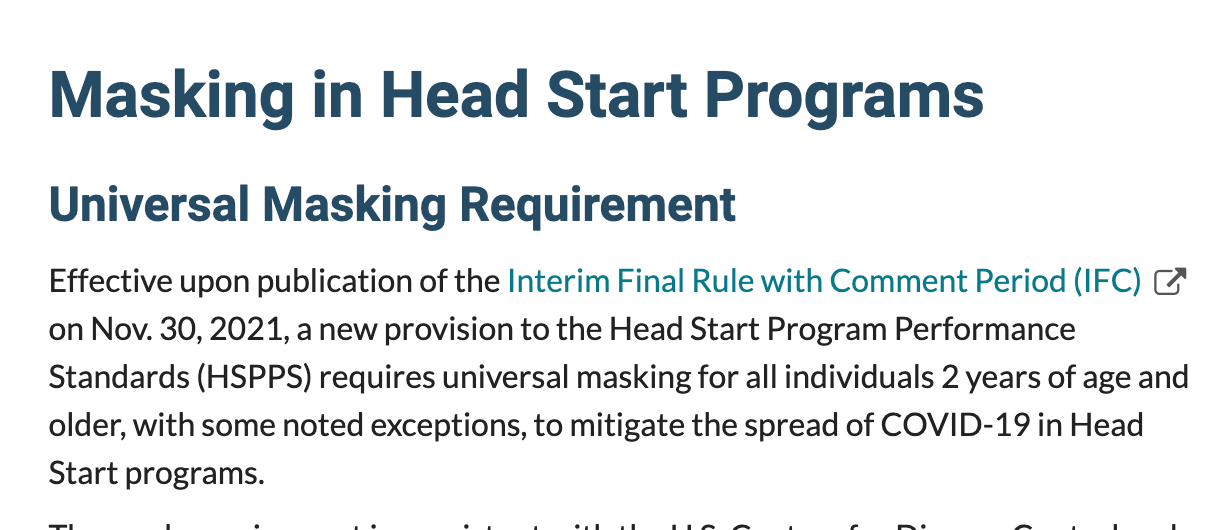
I think we can expect by the new school year (fall, 2022), the use of masks in toddlers and young children in Headstart will be dropped if the child is vaccinated.
They will essentially require vaccination of our youngest and most impoverished children. Even though the vaccinations do not stop transmission and spread. Even though the vaccines have not been fully tested and are neither safe or effective…
When does it end?
*
This all gets kind of old doesn’t it? But that doesn’t mean that we should not pay attention or that we should just comply. Because we can’t afford to ignore these absurd bureaucratic policies that are grounded far more in bizarre ritualistic behavior based on myths, and the need to control and intimidate, than they are in scientific facts. We have to protect our precious children. We have to protect their physical and mental health. We have to ensure that they have every opportunity to develop normally.
The bottom line – this fight isn’t over yet. Our children are still being forced to wear masks if they are very young or in many areas in the USA. That is eight hours of continuous mask use while at school or in the case of summer camps, it could literally mean 24 hours a day. Just think about that.
This is not ok. The HHS can not be allowed to continue to require and/or recommend the use masks for children.
But back to the parent in my opening paragraph, whose child was being required to wear a mask. In response, I can only answer as to what would I do if I had children in a public or private school or camp that required masking. The answer is simple. My family would not comply. That means my children would not go to that venue. Even if it meant losing those fees. Masking of children is not ok.
Right now, parents are lucky because there are so many options for home, private and co-op schools. Social media abounds with opportunities to educate children without paying a fortune and without enrolling in public programs. But there is no question, educating our children without attending public institutions is hard and will require great sacrifice. I urge folks to reach out to relatives, friends and family for help. Most people have more support than they realize. The community must help to protect our children.
We can not stop our out-of-control government, but that does not mean that we do not have choices.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Featured image is from Robert Malone