

All Global Research articles can be read in 51 languages by activating the Translate Website button below the author’s name.
To receive Global Research’s Daily Newsletter (selected articles), click here.
Click the share button above to email/forward this article to your friends and colleagues. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
***
What would have happened without a mandatory ‘stay home, save lives’ COVID lockdown protocol? Was there ever a cost-benefit analysis performed by any government in any country? How were populations cajoled into accepting the official COVID narrative?
These are just some of the questions that spring to mind when listening to Bhaskaran Raman, an associate professor at the Department of Computer Science and Engineering at the Indian Institute of Technology Bombay.
His recent 70-minute presentation on the global approach to COVID is extremely insightful. The lecture took place at the Dr D Y Patil Medical College, Hospital & Research Centre in Pune.
Raman takes us on a journey. Piece by piece, he dismantles the official narrative pushed by governments and media. He shows how, among other things, ‘science’ was manipulated to fit a predetermined policy which included a rejection of natural immunity in favour of ‘stay home, save lives’ policies, how prevailing pandemic protocols were trashed, how fear was ramped up by 24/7 scare stories and the misuse of PCR tests in order to maintain the illusion of a ‘deadly pandemic’ and how lockdowns did more harm than good.
Three years on from the start of COVID policies, we have witnessed mandated vaccine protocols and various methods of coercion to increase uptake, the destruction of small businesses and surging profits for the world’s billionaires and hundreds of millions pushed into poverty resulting from restrictions and lockdowns.
We also see a major debt crisis with IMF/World Bank loans tied to austerity conditions, millions of vaccine adverse reactions (including death) and the WHO pushing for an authoritarian global pandemic treaty – based on the house of cards described below and involving many of the figures who helped construct this medical tyranny – which will ride roughshod over national sovereignty.
For those who don’t have time to watch the presentation, what follows is a summary (edited and sometimes paraphrased) with screenshots.
Readers are urged to watch the presentation in full here.
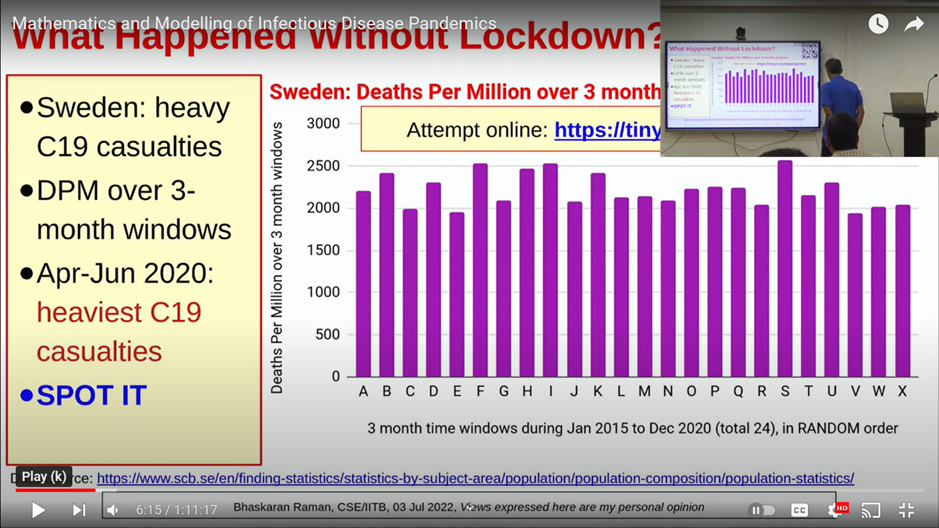
Raman begins by discussing the mortality rates in Sweden, a country that never imposed a lockdown.
*
Sweden: spot the pandemic?
I decided to look at the data. This is openly available. You can do this in 10 to 15 minutes of spreadsheet work from the link on Sweden’s official health website.
In this graph (below), what I did was I took three-month windows of time. There are four such windows in each year and I took data of six years starting from 2015.
In the country that did not lock down, you cannot spot the pandemic.
But some say Sweden cannot be compared to other countries as it has among the best healthcare facilities in the world, which is true, and Sweden’s population density is very low – much lower than most other countries.
So, I took a look at the polar opposite of Sweden in terms of population density, which is Dharavi, the largest slum in Asia (in Mumbai). The healthcare facilities there are extremely poor of course.
Note: Raman then goes on to state that Dharavi was under lockdown, and no one was allowed to leave the area. People were locked in and living on top of each other with limited chance of social distancing. Yet the COVID death rate was an eighth of that of the USA and UK.
Impossible advisories were saying stay six feet apart – impossible in a 10-foot by 10-foot room with a family of four or five and houses so close to each other.
Note: He looks at the lockdown in India and traces the trajectory of COVID and finds no connection between lockdown and the severity or relaxation of restrictions.
Here is a study (below) which looks at 188 countries, pretty much the entire world, and it looks for correlation between stringency of the measures measured as per a metric to the stated mortality rates.
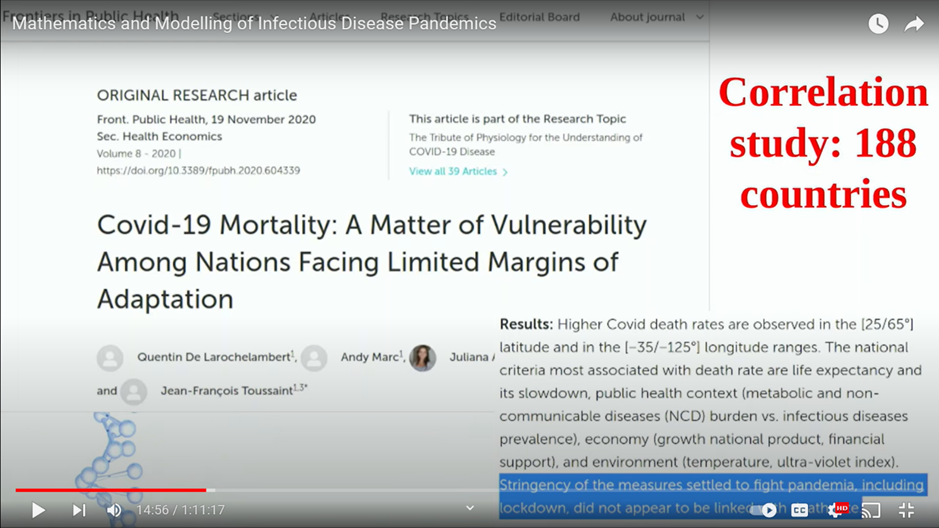
What they concluded was that the measures, including lockdown, did not appear to be linked to death rate – the mathematical correlation was near zero.
If the messaging ‘stay home, save lives’ was indeed correct, you would expect a huge death rate in countries which did not lock down versus countries that did lock down.
That wasn’t the case; the correlation was in fact the reverse. The more stringent the measures, the higher the COVID mortality.
You have to ask how lockdowns came to be the narrative being pushed.
Prevailing pandemic guidelines trashed
Lots of countries had written guidelines – pages and pages of written guidelines of what to do in this exact situation.
These guidelines (below) were written in 2019.
There are several rows on what to do in case of a moderate pandemic, what to do in case of high severity and what to do in case of extraordinary severity, and the specific thing I want to highlight is the last row which says not recommended under any circumstance.
Okay, so let us look at what is written under not recommended under any circumstance.
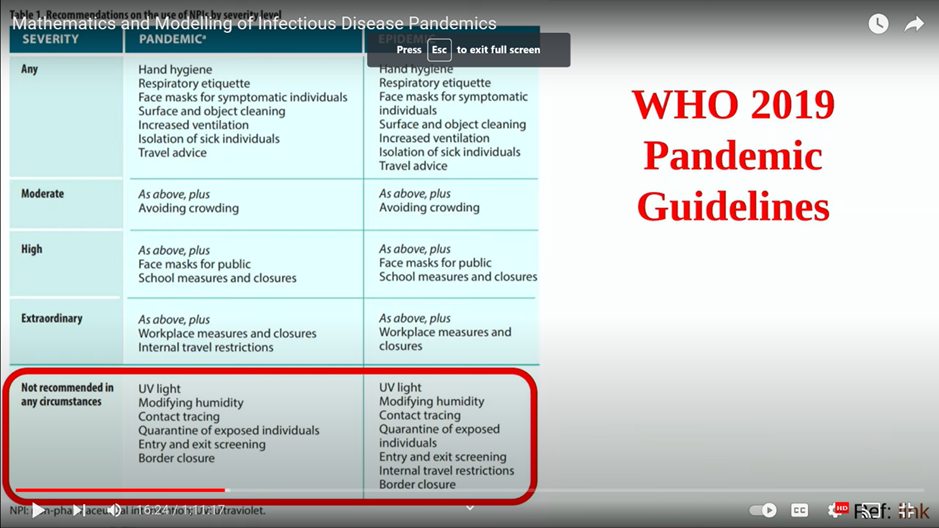
Contact tracing is not recommended under any circumstance. It says you do not have to be quarantined. The quarantine of exposed individuals is not recommended under any circumstance. If you think about it, lockdown is basically quarantine of everybody. Entry and exit screening and a border closure too (are not recommended).
We have a table from the US CDC guidelines written in 2017. I’ll read this out – “CDC might recommend voluntary home quarantine of exposed household members.” But what we had throughout the world was state mandated stay-at-home orders.
So, we now have to ask – how did this come to be when there are written guidelines for handling this exact situation. Why were the entire guidelines basically thrown into the waste basket?
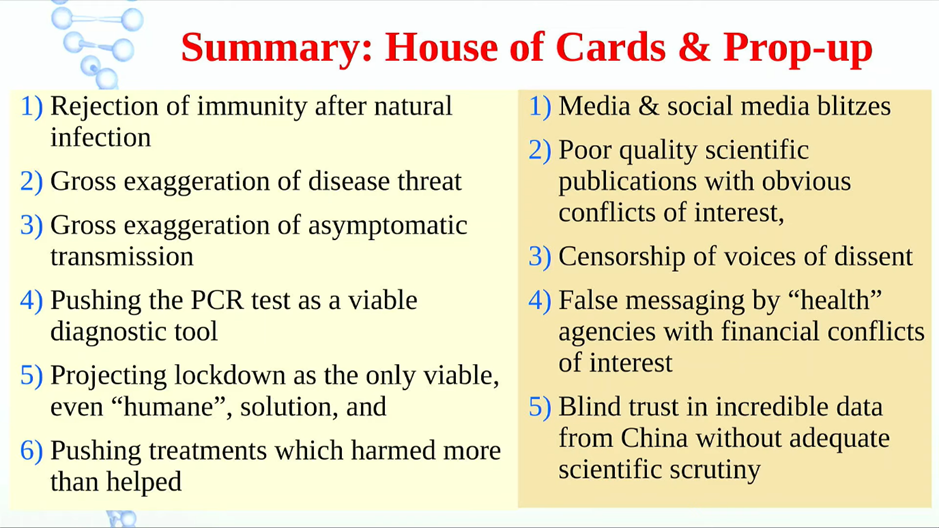
Novel approaches were taken. I have divided these into six different parts.
First is the rejection of immunity after natural infection. Second is wild exaggeration of the threat posed. Third – gross exaggeration of the role played by asymptomatic transmission. Four – the PCR test was pushed as a viable diagnostic tool. Five – lockdown was being projected as the only viable solution. Six – I’ll touch upon treatments which actually harmed more than helped.
Rejecting natural immunity
Note: He then notes that, early on, the only place that shows lockdown worked – supposedly bringing COVID deaths to zero – was China.
Since then, no other country has been able to reproduce this result, so you have to question either the data – or some other influence.
Note: The presentation discusses natural immunity after infection. It was being portrayed from the beginning that ‘no one is safe until everyone is safe’. Raman shows a screenshot of how the definition of herd immunity was conveniently changed by the WHO in favour of an all-or-nothing vaccine – sit at home and wait for the jab. This new definition justified lockdowns and the notion that you are only safe until everyone is safe (vaccinated).

The Lancet also promoted a similar message.
Scientists were calling for virus elimination – same as The Lancet. No COVID. So, you want to reduce COVID to zero. Of course, by that time also it was known that there was community spread all over. A lot of the people don’t even show symptoms, and there were also non-human species to which the virus had spread. The goal of virus elimination is not just impossible. It’s close to delusional: you cannot eliminate a respiratory virus which has already spread so widely across the planet even to other species.
Nearly two-thirds of the people in slums already had antibodies (natural herd immunity).
Note: Raman says the death rate in Dharavi was much lower than elsewhere, indicating the beneficial effects of natural immunity.
Threat of COVID: wild exaggeration
So, let me begin with what was happening in early 2020. Thanks to this technology called social media, there were all sorts of videos going around and quite a few of them in mainstream media.
Note: He provides examples of staged events, mainstream media misinformation (outright lies) and fear mongering, whether emanating from China, the US, Italy or beyond.
WHO Director General Ted Ross claimed that the fatality rate of COVID was 3.4 per cent, whereas the seasonal flu which we are used to kills far less than one per cent. He gave that statement – the entire world media ran with it. The fatality rate of seasonal flu is only 0.1 per cent.
It looks very dangerous obviously – 30 times more dangerous than what we are used to is enough to scare anybody. But there was only one problem with this: the comparison was false.
This is a graph which I have taken from Business Insider, which has a very wide reach. In early March 2020, it compared the fatality rate side by side for flu and COVID. Well, this looks scary. If you look at it now, it is still scary, but it is false because it was comparing the case fatality rate of COVID with the infection fatality rate of flu. Striking fear in people’s minds.
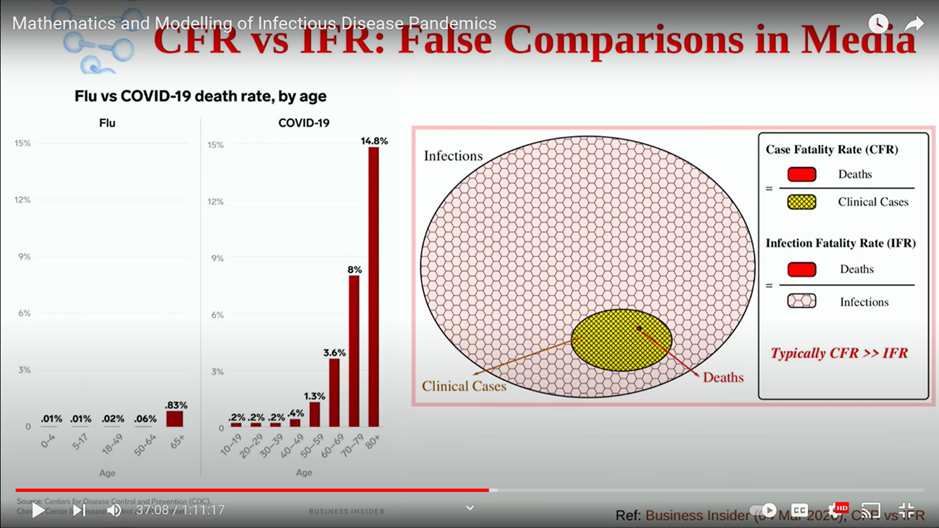
Note: The impact of COVID was heavily overstated (at times, 30-40 times more deadly than it was) in various graphs and by various data dressed up as scientific ‘fact’, and the media wasted little time in scaring the public with this flawed data.
So, this confusion between CFR and IFR was one of the major elements in exaggerating the threat. In turn, this connects with why people accepted lockdown.
The New York Times had a podcast where it compared the fatality rate of COVID with Spanish Flu. Once again, a wild exaggeration. Based on available figures, COVID was about 30 times less dangerous, looking at the US data.
It’s not just a normal exaggeration. It is epic-scale exaggeration.
Boosting fear: asymptomatic transmission
There was also the gross exaggeration of the role of asymptomatic transmission. This was a huge element in making every person looking upon every other person as a disease agent, not as a human. The entire societal fabric was broken because of this.
Evidence for asymptomatic transmission from the beginning was very weak – very shaky.
Media reports fuelled the fear of asymptomatic spread. In July 2020, a report based on investigations from China suggested that people without symptoms could infect others. The strange thing was that when scientists tried to replicate this in other countries outside of China, they could not replicate it.
A paper from May 2020 from Taiwan – they did a contact tracing-based assessment, and they could not find any instance of asymptomatic transmission.
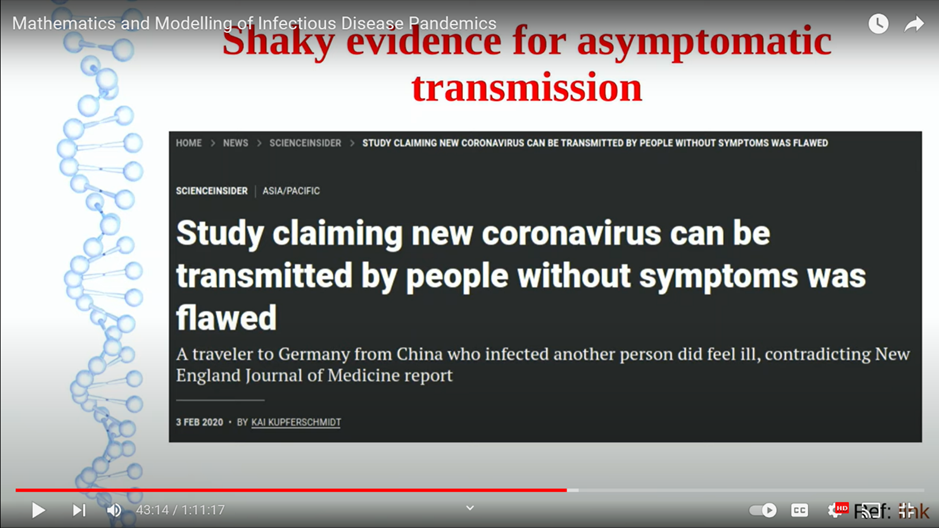
Note: Raman shows that studies coming out of China made the case for asymptomatic spread, but studies conducted in other countries failed to demonstrate this.
Another meta-analysis in mid-December 2020 basically concluded that asymptomatic transmission is statistically indistinguishable from zero. If you think back, this was a basis for the lockdowns – people without symptoms can transmit.
PCR tests: instruments of fear
Let’s look at part four, which is pushing the PCR test as a viable diagnostic tool.
This audience probably doesn’t need any introduction to the PCR test.
Note: He describes how the PCR test was implemented as the go-to test for COVID at the ‘speed of science’. A group of researchers submitted a paper on the efficacy/usefulness of the PCR test in January 2020 – within four days it was published in a scientific journal.
This was accepted within one day. So, this was the ‘speed of science’.
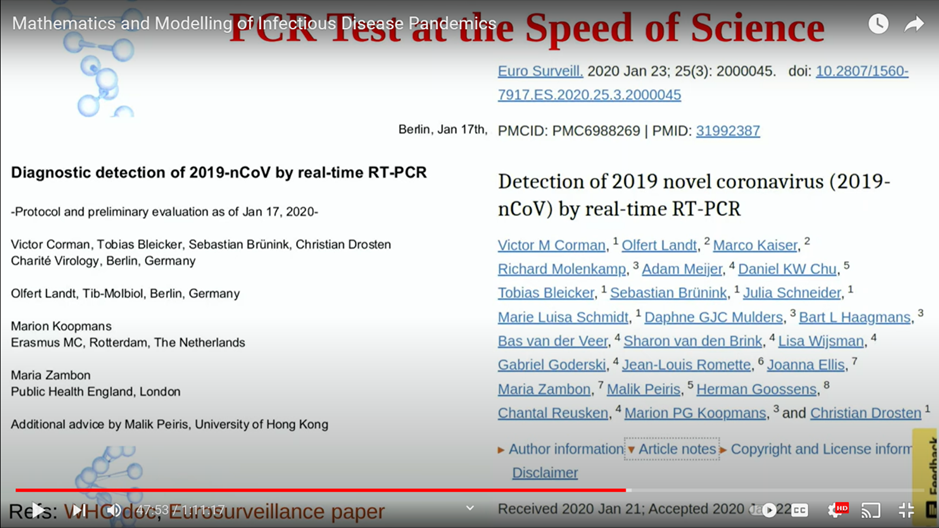
Note: How long does it take to conduct research with scientific rigour? Aside from that – how long would it normally take to undergo proper peer review?
A lot of people complained about this (‘speed of science’): they were given the reasoning that well it was an emergency and hence we had to fast track. Okay, sounds reasonable, except that if you look back at the data in January outside of China, I think the number of deaths were in probably single digits or maybe double digits. How can they conclude that an emergency was about to happen?
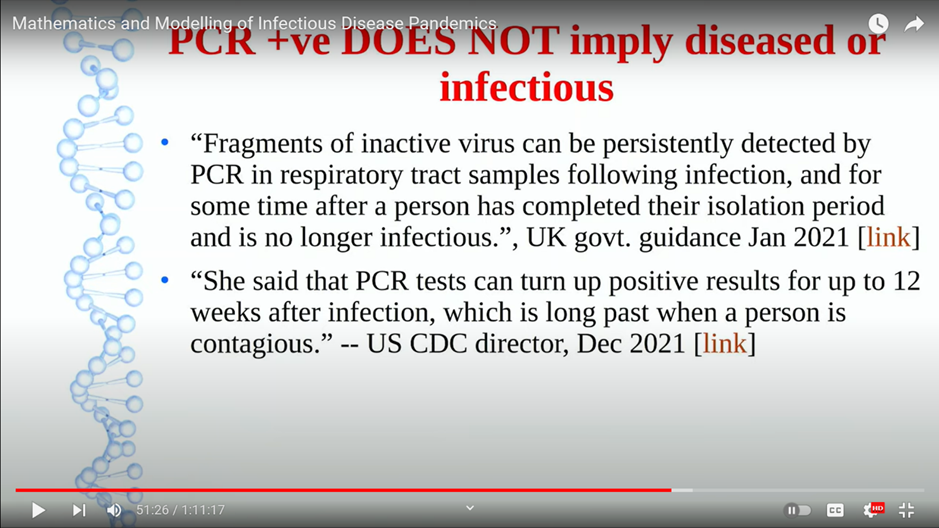
Viral fragments can remain in the body for up to 90 days and the PCR test is only detecting viral fragments. It’s not detecting live virus. This was admitted by the US CDC director in December 2021.
If you go around looking for respiratory viruses, especially in hospital settings among people who have died, you will find them.
This is a paper (below) which looked at detection of respiratory viruses using PCR test in people who are dead people from 2017 from Spain. It found that nearly half the people had respiratory virus.
However, prior to their death, only seven per cent were detected with the respiratory illness, which means that PCR positive does not mean it is the cause of death.
For the first time in human history, a person doesn’t have any symptoms and there is no doctor in the picture – but disease is detected. It’s incredible.
We had asymptomatic cases. What does that mean? An asymptomatic case means the person is healthy. I mean, of course, people in the street had figured it out. If they are perfectly healthy, they are more afraid of getting forcible tests done. Why do you want to get your entire building quarantined?
I’m sure you all know the PCR test was designed as a research tool. It’s not for virus detection in the absence of a doctor.
You cannot have politicians using PCR tests to label people as diseased and shutting off entire cities. That doesn’t make any sense at all. And the WHO does not have any clinical diagnosis protocol to this day. It cannot because the symptoms are overlapping with other conditions. So, the tool that did the test which has been extensively used – there is no false positive rate. Nobody Knows the false positive rate for disease detection or infectiousness. There are some studies for the presence of live virus, but these two (disease presence, infectiousness) are just impossible. There have been no studies because there is no clinical diagnosis protocol.
The projection of PCR test as a viable diagnostic tool again played a huge role in ushering in lockdowns because they can just ramp up testing and show people as positive. It’s actually dead virus. The person is perfectly safe and healthy.
Lockdowns – China as the template
Let’s come to the fifth part – where lockdowns were projected as the humane solution. The WHO from the beginning had been praising the Chinese Communist Party’s methods for fighting coronavirus. This is a quotation from 30 Jan 2020
“We welcome the leadership and political commitment of Chinese government and its commitment to transparency.”
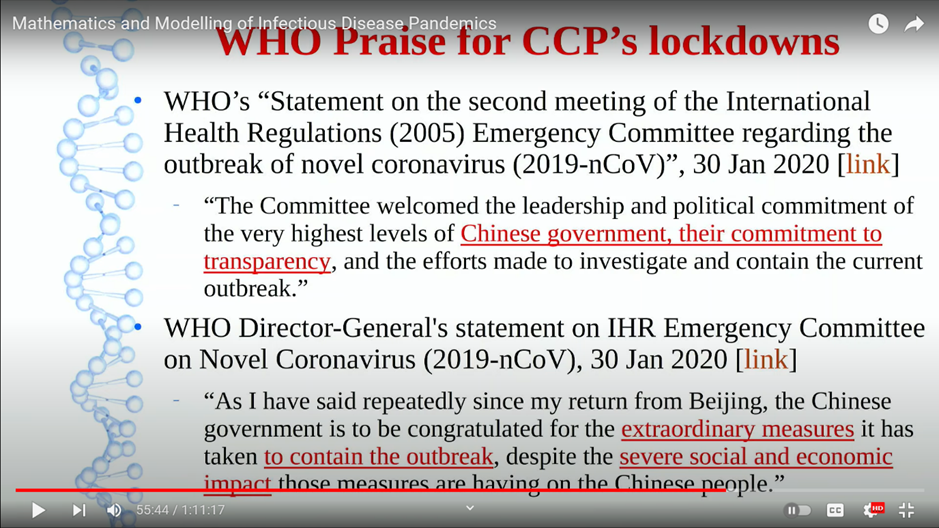
If I have to think of a government which is transparent, the last country I’ll think of is China. For decades it’s been completely non-transparent. No journalistic freedom, no foreign journalists allowed. And then here, we have the WHO praising it: how can a government suddenly turn transparent overnight? It’s incredible.
So, this WHO praise for the CCP was going on for a long time. Then Canada’s members of parliament called one such WHO official – this is a picture of Bruce Aylward, one who was going around showing the China data. They summoned him for an investigation. He didn’t go. The WHO forbid him from testifying (in front of a health committee).
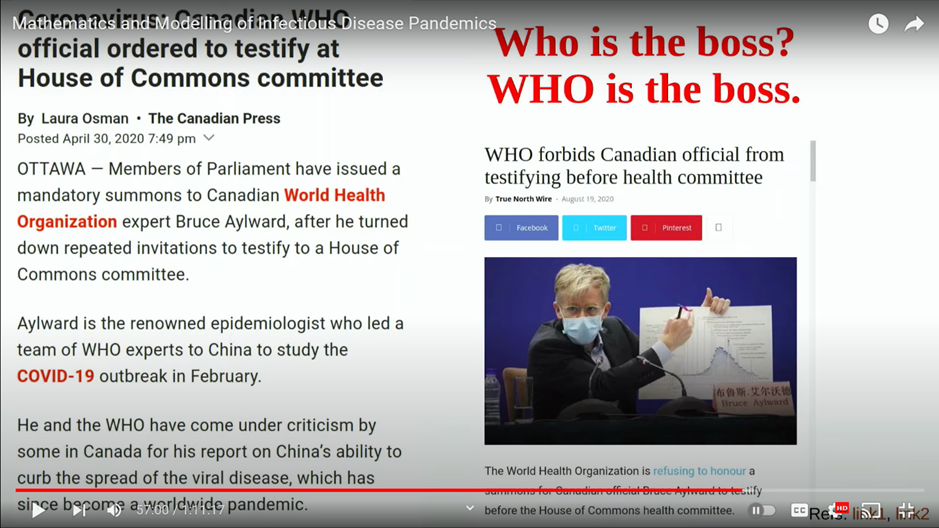
The WHO is the boss. Are they the elected representatives of Canada? The WHO was praising the CCP’s transparency while being non-transparent itself.
And then we have the modelers like Neil Ferguson from Imperial College London, one of the most reputed colleges in the world, basically lending implicit credence to this graph (below) saying that this graph resulted because of China’s measures to control COVID 19. This was used to bring in lockdowns in the UK.

As a reminder, this was the graph which they were lending credence to – a graph which no other country has been able to reproduce.
The New York Times, in one of its rare moments of actual journalism, had a series of articles calling out China’s social media campaign. It had lots of bots, fake accounts flooding the internet, praising the CCP’s methods of handling the pandemic.
Note: Raman also notes that the journal Nature was also using China as a template for its discussion of lockdowns.
‘Consensus’ through censorship
Basically, what’s going on is information warfare. While China was doing this kind of information manipulation, the US was not far behind in terms of its own censorship.
In early October 2020, three epidemiologists came out with the Great Barrington Declaration as a position statement against lockdowns, saying they are not going to do anything to impact the disease. You need to do focused protection. Focus on those who are actually vulnerable. Otherwise, you’re going to have lot of collateral damage.
Fauci and Collins, who were at high places in National Institute of Health, which was sitting on lots of funding at that time, collaborated with social media companies to censor the Great Barrington Declaration.
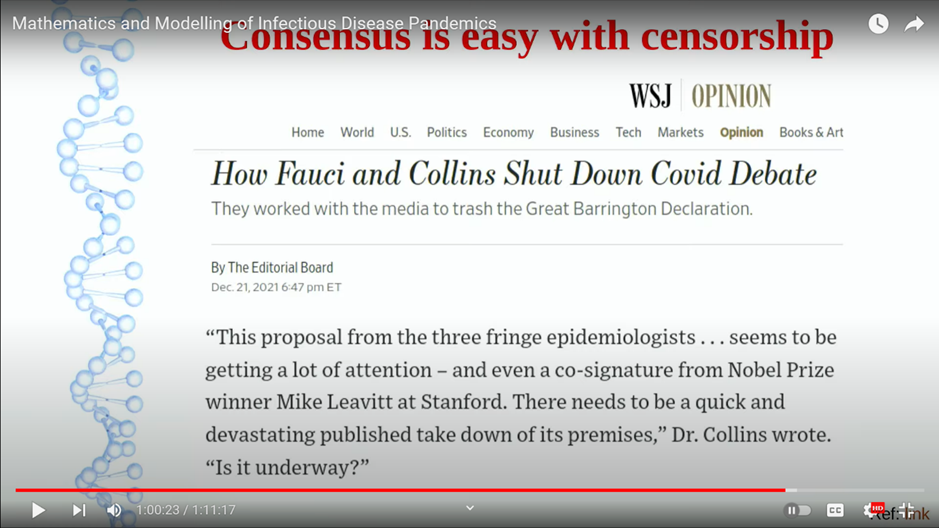
So, the exact wording is there needs to be a quick and devastating published takedown of its premises. This was revealed in an email via a freedom of information request. Collins wrote to – I don’t remember exactly to who – but he was calling for social media companies to take down a Great Barrington Declaration, so it looked as though there was scientific consensus that lockdowns were the only viable solution. Consensus is easily shown when you have censorship.
Containment or doing harm?
This is part six. There were lots of documented instances of treatments which we now know were causing more harm than helping. Early on, the WHO was recommending early mechanical ventilation, again based on studies from China, and then later on after the huge number of deaths in New York.
There were papers saying this is clinically not the right way to do things. There was a incredible article in the Wall Street Journal in December 2020. I’ll read this out because it’s heart wrenching in many ways. One of the doctors, a doctoral nurse, says we were intubating sick patients very early, not for the patient’s benefit but in order to control the epidemic and to save other patients. That felt awful.
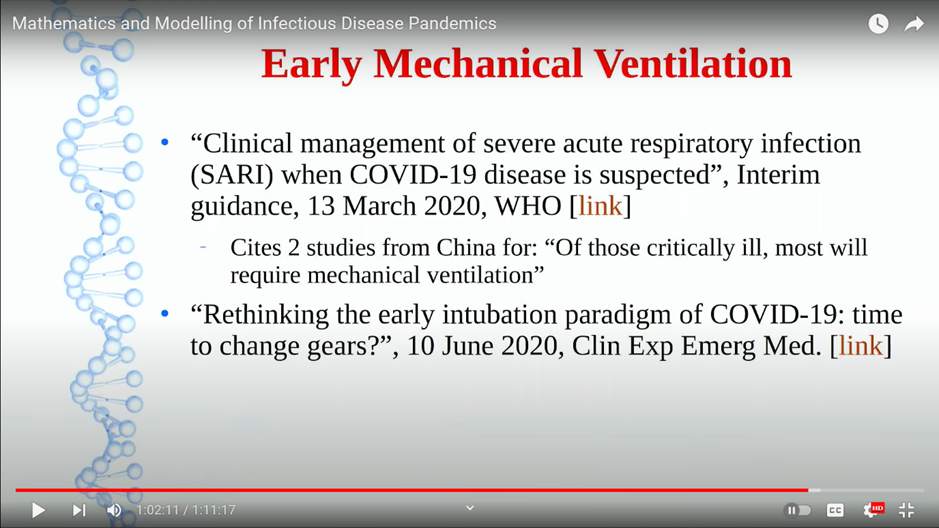
This was the containment narrative that was pushed. Who knows how many people fell prey because of this kind of wrong intervention. Chosen not for the benefit of the patient but for so called containment.
And then we all know about the panic which happened in 2021 during India’s second wave. There is a journalistic piece in The Mint which reported on a certain batch of remdesivir which was later found to be very toxic. People were craving for it. Who knows how many came from this bad batch and basically killed people.
We really don’t know how many were actually killed by the virus versus how many by this kind of bad medication. Publications were even asking whether there was any benefit at all for its use in COVID. Statistically, there doesn’t seem to have been any benefit.
Lockdowns: destroying health and wellbeing
And what about the lockdown?
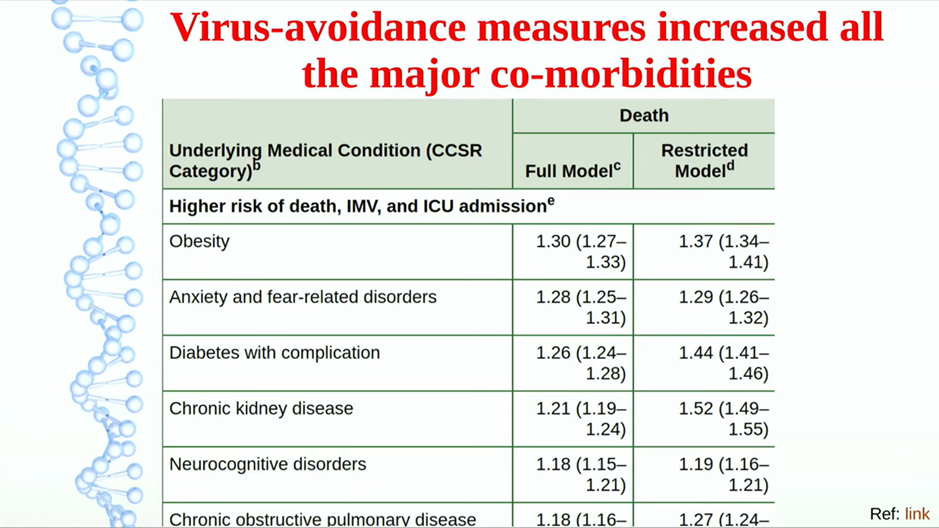
The CDC noted obesity was the topmost comorbidity, second was anxiety and third was diabetes.
Now, what happened because of lockdown? Obesity increased. In Australia, I believe the average weight increase was like three kilos. A good number of people would have increased much more than that.
Anxiety, of course. 24/7 for two years. Scare, scare, scare. Any time you saw the news, it was anxiety and fear. If there is a real panic situation, you have to calm people down to reduce the mental health toll.
People were denied walking, exercise, gyms closed, playgrounds closed, no morning walks. What happens to people with diabetes?
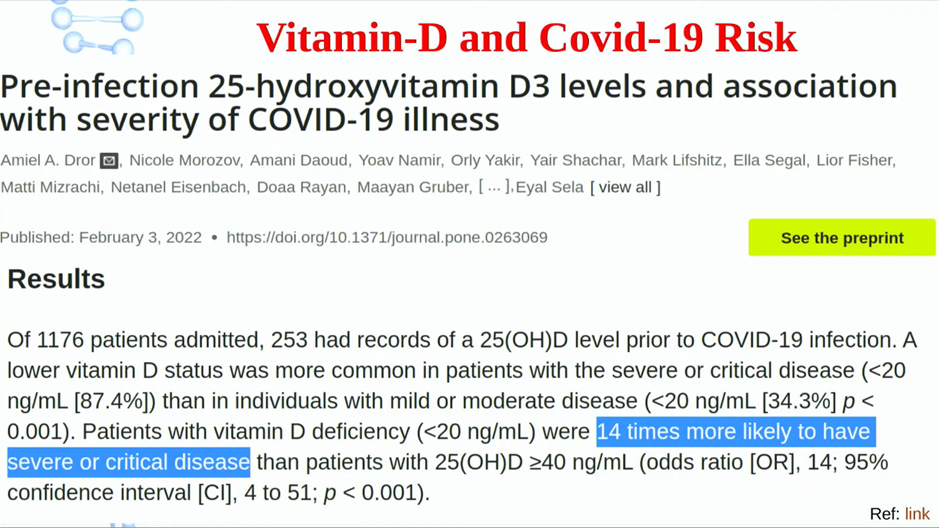
And then this is another big one – vitamin D deficiency if you shut down an entire population for an entire year saying, ‘stay home, stay safe’. You would expect that vitamin D levels will go down because sunlight is important for vitamin D. This Israeli study documented an increase in risk of 14 times for COVID severity because of vitamin D deficiency.
So, lockdown itself, far from being a solution, was in fact counterproductive in many ways.
It didn’t save lives, it just postponed deaths perhaps and then probably increase the toll much more.
So here (below) is a summary of the lockdown house of cards and the mechanism used to prop up the house of cards.
*
Note to readers: Please click the share buttons above or below. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
Renowned author Colin Todhunter specialises in development, food and agriculture. He is a Research Associate of the Centre for Research on Globalization (CRG) in Montreal.
Featured image is from Medical Tyranny
 Read Colin Todhunter’s e-Book entitled
Read Colin Todhunter’s e-Book entitled
Food, Dispossession and Dependency. Resisting the New World Order
We are currently seeing an acceleration of the corporate consolidation of the entire global agri-food chain. The high-tech/big data conglomerates, including Amazon, Microsoft, Facebook and Google, have joined traditional agribusiness giants, such as Corteva, Bayer, Cargill and Syngenta, in a quest to impose their model of food and agriculture on the world.
The Bill and Melinda Gates Foundation is also involved (documented in ‘Gates to a Global Empire‘ by Navdanya International), whether through buying up huge tracts of farmland, promoting a much-heralded (but failed) ‘green revolution’ for Africa, pushing biosynthetic food and genetic engineering technologies or more generally facilitating the aims of the mega agri-food corporations.