

The US media is relentlessly spinning fear, panic and despair, with the endorsement of “authoritative” American scientists. “The new coronavirus could kill millions across the United States”, according to Dr. Kathleen Neuzil a specialist in vaccines at the University of Maryland School of Medicine. (CNBC, March 18).
The media routinely exaggerate the health impacts as part of their fear and panic discourse.
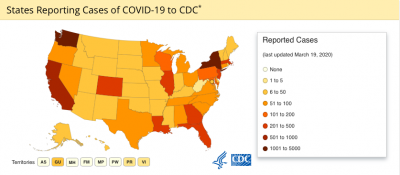
Lets look at the figures. The latest coronavirus data in the U.S released by the CDC on March 18, 2020 are as follows:
- Total cases: 10,442
- Total deaths: 150
- Jurisdictions reporting cases: 54 (50 states, District of Columbia, Puerto Rico, Guam, and US Virgin Islands)
UPDATE: Since the publication of this article, the reported CDC total cases and total deaths have increased substantially.
- Total cases: 15,219
- Total deaths: 201
March 20 figures
According to latest media hype, citing and often distorting scientific opinion (CNBC)
Statistical Models by Washington think tanks predict a scenario of devastation suggesting that “more than a million Americans could die if the nation does not take swift action to stop its spread as quickly as possible”.
One model from the Centers for Disease Control and Prevention (CDC) suggested that between 160 million and 210 million Americans could contract the disease over as long as a year. Based on mortality data and current hospital capacity, the number of deaths under the CDC’s scenarios ranged from 200,000 to as many as 1.7 million. (The Hill, March 13, 2020)

.
Who to Believe?
The most commonly reported symptoms [of COVID-19] included fever, dry cough, and shortness of breath, and most patients (80%) experienced mild illness. Approximately 14% experienced severe disease and 5% were critically ill. Early reports suggest that illness severity is associated with age (>60 years old) and co-morbid disease. (largely basing on WHO’s assessment of COVID-19 in China)
 The Hill, March 19, 2020
The Hill, March 19, 2020
And then these “mild symptoms” of COVID-19 are used as a public health justification for the closing down of entire countries, precipitating large sectors of the World population into unemployment, poverty and despair.
Bear in mind that, the COVID-19 hits the 60 years+ elderly (most of whom are not part of the labor force), particularly those who do not have adequate health coverage. In the US the COVID-19 deaths are largely recorded in the 70 years + range. The confirmed death rate from COVID-19 is 1.4% of total “confirmed” and “presumed” cases (CDC data).
Compare “the Mild Illness and Recover in Two Weeks” of COVID-19 (barely acknowledged by the media) to the devastating social and economic consequences of the lockdowns ordered by powerful financial interests.
 Millions of Americans have lost their jobs, thousands of small enterprises across the land have been spearheaded into bankruptcy. Millions of families have lost their lifelong savings as a result of the collapse of stock markets. Precipitated into a debt trap, they may lose their homes.
Millions of Americans have lost their jobs, thousands of small enterprises across the land have been spearheaded into bankruptcy. Millions of families have lost their lifelong savings as a result of the collapse of stock markets. Precipitated into a debt trap, they may lose their homes.
And that scenario will not “recover” in two weeks. It’s a long term depression. What we are dealing with is the destabilization of the US economy and an engineered transfer of billions of dollars of money wealth.
COVID-19 Recovery Rates
The CDC Data tabulates both “confirmed” and “presumptive” positive cases since January 21, 2020. Yet what it fails to mention is that among the confirmed and presumptive cases, a large number of Americans have recovered. But nobody talks about recovery. It does not make the headlines.
In China, there is a distinction in the data between “confirmed cases infected” and “confirmed cases recovered”. The recorded recovery rate in China is of the order of 80% since the outbreak of the epidemic in Wuhan in early January. (See Xinhua, March 19 2020)
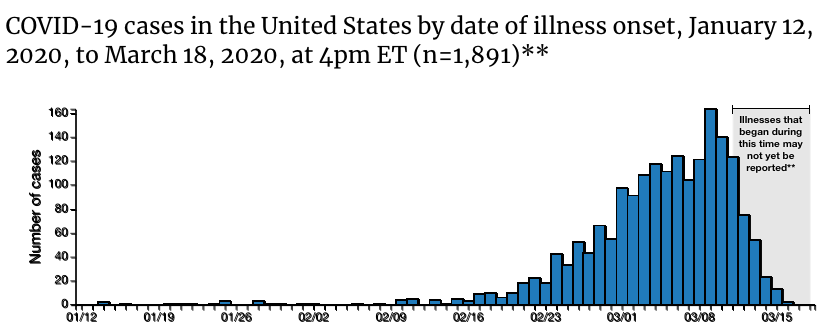
In the US, the hike in “confirmed and presumptive cases” started in late February to early March (see graph below).
Applying recommended medication, the recovery rate –according to the WHO report cited above– would be of the order of two weeks for most patients under 60 (a longer period of recovery for the population group over 60).
What this suggests is that the COVID-19 public health crisis in America could be brought under control in a matter of months. But if that were to happen, it would undermine the implementation of Big Pharma’s Vaccination project.
There are serious difficulties in the testing process. Reliable test kits are “in short supply”.
Presumptive vs. Confirmed Cases
According to the CDC the data presented for the United States 10,442 cases ““include both confirmed and presumptive positive cases of COVID-19 reported to CDC or tested at CDC since January 21, 2020″.
The presumptive positive data does not confirm coronavirus infection: Presumptive testing involves “chemical analysis of a sample that establishes the possibility that a substance [COVID-19] is present“(emphasis added). But it does not confirm the coronavirus infection. The presumptive test must then be sent for confirmation to an accredited government health lab. A confirmatory testing implies “identification of the specific substance [coronvirus] through further chemical analysis.”
It is worth noting that the WHO does not tabulate presumptive data. Its total confirmed cases figure is significantly lower than the total “confirmed and presumptive” cases presented by the CDC.
WHO figures for the US: 3586 total confirmed cases plus 1822 new confirmed cases. (March 16, 2020)
(discrepancies with CDC data may also be due to delays in data processing).
State and local data are at odds with the figures published by both the WHO and the CDC, they are invariably much higher.
There are flaws in the process of of COV-19 testing and data collection by local, State and CDC.
The CDC data does not include “testing results for persons repatriated to the United States from Wuhan, China and Japan”. Why?
The above statement suggests discrepancies in the overall assessment of confirmed cases. Why is the publication of the data pertaining to persons repatriated from China and Japan withheld by the CDC? Is that data classified?
Officially, according to the WHO and the CDC the coronavirus takes its origin from China which suggests that all the cases in the US took their origin in China. Why then are these estimates not included?
The White House ordered meetings where officials discussed the coronavirus to be classified, … Federal health officials were directed to keep dozens of meetings that started in mid-January, including discussions on the scope of infections, quarantines and travel restrictions confidential, … According to the sources, those without security clearances were not permitted in the high-security room, typically used for military and intelligence operations, at the Department of Health and Human Services (HHS), where the meetings took place. (The Hill)
And what do the pathology reports of the lab tests pertaining to imported China viruses reveal? What strains? Classified.
Trump call it the “Chinese virus”: Are the COVID-19 “confirmed case” of imported “foreign” infections from China/Japan the source of “transmission” to those COVID-19 cases recorded across the United States? There is no available evidence to that effect.
Seattle, “America’s Wuhan”?
Examine the CDC Map below (March 19). The largest concentrations of confirmed and presumptive positive cases are in New York State (NYC Metropolitan area) and the State of Washington (Seattle).
.
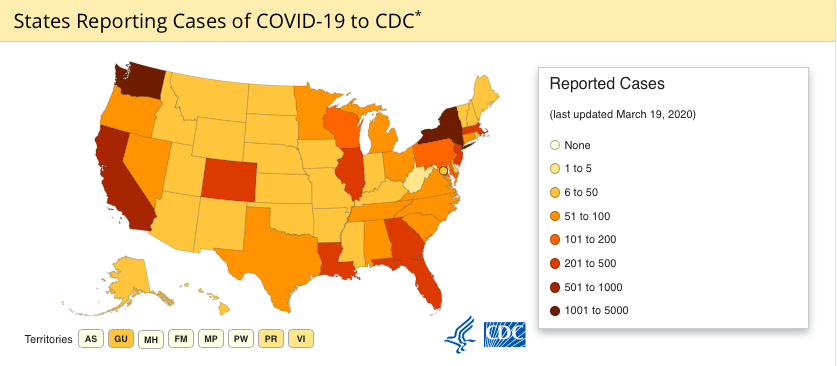
Data problem, causality? The State of Washington accounts for more than ten percent of the cases.
44.7% of the recorded COVID-19 deaths in the United States have been recorded in Washington State. Most of the cases and deaths are concentrated in Seattle.
The population of Washington State is 7.5 million, barely 2.2% of total US population (330 million).
We will not speculate on the data issue. It is a matter which has to be carefully investigated.
As of March 15, 67 deaths from COVID-19 have been reported in Washington State. (total for USA; 150, according to CDC)
According to Washington state data, there are 1,187 confirmed cases of COVID-19. (Not including presumptive cases).
“And King County officials said there are now 562 confirmed cases just in King” (March 18). Most of the deaths are elderly (70s to 90s), many of whom mysteriously died at Life Care Center. Out of 67 deaths, 30 were recorded at the Life Care Center.
What is significant is that none of the recent CDC and state level reports intimate that U.S. cases of COVID-19 infection have been transmitted from China directly or indirectly.
Note
Bear in mind the methodology of CDC estimates is defined as follows: State and local public health departments are involved is testing and data collection independently of the CDC. “In the event of a discrepancy between CDC cases and cases reported by state and local public health officials, data reported by states should be considered the most up to date.” (CDC, March 18, 2020)