


Dear Sirs and Madams,
I am an independent scientist of over 30 years experience leading research into new medicines, operating up to Vice President and head of Respiratory Research at Pfizer, a US pharmaceutical company and founder and CEO of Ziarco Ltd a biotechnology company sold to Novartis in 2017.
As an independent I am less constrained than academics and commercial persons. However, I have applied the same rigour to analysing the pandemic since March as with any of my former projects.
In brief:
- I am certain the pandemic is over and was over before the end of June.
- There was a clear peak of excess deaths in spring. COVID-19 clearly caused many deaths, mostly of the elderly and already ill.
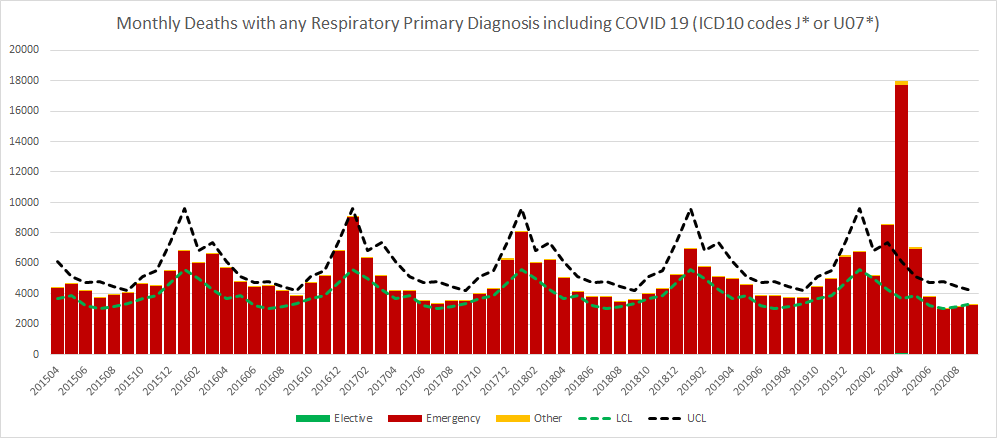
- Turning to late summer and into the autumn – despite exaggerated claims that there is an ongoing full-blown pandemic, there are still FEWER respiratory deaths than at the same time periods in all five of the years since 2015. The below shows monthly deaths with any respiratory primary diagnoses including COVID-19.
There is a small and potentially growing all-causes excess mortality signal. I am working with a pathologist and our evaluation so far shows that these excess deaths are inconsistent with being COVID-19. In short, they are not dying from respiratory illness, but from heart failure and from cerebrovascular accidents such as stroke and diabetes. An awful realisation I have is that these excess deaths are just the sort you would expect if you take a mixed population, deprive them of easy access to the healthcare system for seven months and keep them stressed.
Looking at data obtained from contacts within the NHS, we do not have hospitals full of respiratory patients to any greater extent than usual for November. There are always hotspots and we know Liverpool is one such today. Again, the evidence is against this being due to COVID-19. And to repeat, we have not had excess respiratory deaths since the spring event itself. Liverpool and other cities and towns nearby have additional capacity and ‘surge capacity’, if required. The NHS as a whole is not in crisis and there is nothing to suggest it is about to be. I also checked with a colleague regarding intensive care beds. While an increasing number of their occupants have tested positive for COVID-19, intensive care beds are at exactly normal loadings for the time of year, i.e. 82%. I believe those COVID-19 diagnoses are mostly or all incorrect. We have tested well over 30,000,000 people. It wouldn’t be surprising if lots of people get a false diagnosis from a PCR test.
Antibody prevalence in the blood of those surveyed periodically is falling steadily and has been since its peak in the spring, when the virus was moving very fast through the population, infecting perhaps hundreds of thousands per day at its very peak. That antibodies are falling was last week wrongly touted as problematic and suggested immunity was fading. That’s the wrong interpretation. The human body does not maintain high levels of antibodies which are not needed. Consequently, steady falls in prevalence of antibodies is a clear signal that people are no longer encountering the virus. I believe that insofar as it is still present, it has become endemic at low levels and represents no threat to the health of the nation.
As someone experienced at reading into adjacent areas of science which I have done time without number since obtaining my PhD in respiratory pharmacology in 1988, I was always confident that the population would speedily attain ‘community immunity’. This is what I believe has happened as detailed in my article “What SAGE has got wrong”.
In my view – probably because SAGE lacked cellular and clinical immunologist expertise earlier this year and at no time during this event has it seconded a pathologist or an expert generalist such as myself – they’ve made a series of terrible errors which continue to infect policy to this very day. If such experts had been consulted, our advice would have made a huge difference, not least to the starting assumptions which are widely criticised as outlandish in the scientific community. In addition, we could have “sense checked” some of the more perplexingly unlikely predictions, such as 4,000 deaths per day.
The most fundamental error SAGE has made was to ignore all evidence of the very existence of prior immunity in the population on the spurious grounds that this was a novel virus. This virus is in fact related to four common-cold producing coronaviruses in general circulation and it has been shown unequivocally that a sizeable proportion of the peoples of at least Europe and North America possess T-cells that provide them with some protection against both endemic and novel viruses.
This virus is a serious threat to a low proportion of the elderly, especially if they are already ill. This description of the most vulnerable accounts for the vast majority of Covid deaths and the median age of those who’ve died of COVID-19 is slightly older than the median age of those who died of all other causes. However, the majority even of this elderly group survive infection. Overall, the lethality of the virus is now known to be very close to typical seasonal influenza. Notably, in relation to risks to the working population, the lethality of the virus in those aged 60 and younger is actually less than seasonal flu.
By using several sets of data I have been able to estimate the proportion of the UK population who have been infected. If you add them to the estimated proportion of the population that had prior immunity, and take account of the fact that young children do not often participate in transmission or become very ill, it is clear that there are far too few susceptible people remaining in UK to support an expanding infection as has been suggested. Instead, the evidence is strong from practical, theoretical and observational standpoints that the nation as a whole and probably most if not all regions in the UK are already protected by community immunity as described by many world leading academic epidemiologists in UK.
I heard with disbelief suggestions that surviving infection might not lead to immunity, or that immunity might only last a few months. Let me assure you, we have known for scores of years that surviving simple respiratory viruses which are neither immuno-toxic like HIV or change their appearance yearly like flu, leads as a rule, not an exception, to long-lived and robust T-cell mediated immunity. Antibodies may play a role but they are not central. That this ordinary virus has become a global media event is simply not justified by its profile.
I have been active on Twitter rather a lot in recent months. I would suggest that the people of UK are now highly suspicious of what is claimed to be happening. Many is the time people have in exasperation said: “This just doesn’t make any sense.” Indeed, what we are being told (that there is a full blown pandemic still underway) does not make sense and while I have no idea why it is being said, it is doubtless incorrect. Ordinary people know that each season’s flu takes perhaps three-to-four months to pass through the whole population. Knowing that SARS-CoV-2 is more infectious, they know that it would take the same or less time to pass through the UK population, not more. Indeed, we know it was in the UK by February. Adding a generous four months takes us to June, where all clinical signs of COVID-19 has disappeared (ignoring PCR test results, of which more in a moment). The rise and fall of Covid deaths in the UK follows exactly the same curve as that of other, highly seeded/infected countries such as Sweden. There is no doubt that we are in the same position as Sweden and it is only the monstrously error-prone and untrustworthy PCR test that suggests otherwise. What SAGE claims is happening is immunologically implausible in light of other data, specifically the shape of the death versus time curve, which shows beyond all reasonable doubt that the pandemic was self-extinguishing.
The PCR testing machinery is, at best, greatly in error and completely misleading. I have good knowledge of mass testing systems. I have always been deeply worried about polymerase chain reaction (PCR) because of its power, not only to find one molecule as small as a broken fragment of viral RNA and amplify it, sometimes by two to the power of 40, through repeated cycling, but also because it can find something that is not there – it can yield a ‘positive’ result even though the virus is not present. The greater the amplification and the higher the number of tests being done each day day – and the lower the expertise of the staff doing it – the higher the probability of error. I was the person who, with a radio journalist, finally pressed Mr Hancock to disclose the false positive rate of the Pillar 2 test, when it was still measuring far fewer tests per day than now. Having established that false positives exist, it is important to know that the rate of these can be small yet, when the prevalence of the virus is low, many or even all the positive results are false. That’s a practical debate for another time.
Yesterday, in response to a written question, the Government disclosed that while attempts had apparently been made to determine the operational false positive rate, it still doesn’t know it. As an experienced lab scientist, I know that when testing capacity is boosted substantially and the staff recruited have less and less lab experiences, there is only one outcome: errors of handling and of procedure. These in turn destroy the integrity of the testing system. The entire response of the UK depends upon the reliability of these tests. I have to tell you quite firmly: at present, it is practically, logically and legally impossible for anyone to be able to tell you what fraction of the positive tests recently obtained are real and which are not. For a range of reasons related to strong evidence that this virus cannot just hover around as it has been suggested and viruses certainly do not perform waves ever, the most secure conclusion is that these results are not to be trusted and are not reliable in any way.
So what I am saying is this. Despite warnings from all sides over months about this test it has continued to be used with increasing ferocity. It’s a medical diagnostic test. On no occasion would such a diagnostic be put into mass testing – in the NHS, for example – without knowing in advance how reliable it is. In terms of proper characterisation, it has NEVER been measured, despite the war-like impact of the test results on the nation and its people. At a minimum, the charge is reckless endangerment. Given all this information, it is literally impossible to guess whether the FPR is 1% or 10%. If even near the latter, there are no “cases” et seq. And there are other reasons to be very concerned about mass testing which I cannot go into today.
In my view, community mass testing is the pathology in the country now – not the virus. It must cease today. Without the ‘cover’ of mass testing, there is no evidence at all that the health of the nation is under any threat whatsoever. That event occurred in spring and our responses to it have been exaggerated and – what is worse – extraordinarily persistent, even when all the evidence says the pandemic has concluded.
I have a colleague who has a half a dozen sets of data all related to the pandemic. These show clear relationships between the data in the spring, all of which illustrated the impact of the virus. However, time after time, these relationships have broken down. The explanation for this is that at least one of the measurements are wrong, and the culprit is the PCR test. This has happened before. In New Hampshire in the USA there was a hospital that was convinced it had a huge outbreak of whooping cough. Physicians, patients and parents were all very worried about the expected deaths. Eventually, an older physician examined some of the patients and did not agree with the diagnosis. Asking the staff why they were so sure it was whooping cough, the answer was it had been diagnosed by the PCR test, the sole diagnostic tool. A review was ordered and this led to culture of the organism from the suspected patients. There was not a single person who actually had whopping cough. No infectious organism was found. What had happened was a now infamous case of a “PCR False Positive Pseudo-epidemic”. That is what I believe we have now in UK and in many other countries using similar technology.
MPs: If you vote for it now, you will condemn more people to suffering and some to death and the evidence does not support this extreme measure for which, even if the virus was circulating as SAGE claims, there is no evidence of benefit.
I urge you to vote against so we can all disclose our evidence that the pandemic is over and the epidemic of PCR testing can end.
*
Note to readers: please click the share buttons above or below. Forward this article to your email lists. Crosspost on your blog site, internet forums. etc.
Featured image is from LS