


Despite its relative invisibility to most people living in the urban Asia-Pacific, endemic malaria occurs across the region. The unique character of Asian-Pacific malaria includes a serious problem of drug resistance, dominance of a particularly difficult species to control and treat, and another that normally dwells in monkeys but often infects humans. Most nations in the region with endemic malaria have called for its elimination by the year 2030. Meeting that ambitious goal will require mobilizing technical and financial resources, and social and political will. Malaria is a formidable foe fully capable of defeating half-hearted efforts to eliminate it.
Introduction
Many well-educated people think of malaria as a single disease that is largely, if not entirely, isolated to the African continent. This includes many living in the enormous urban centers of the Asia-Pacific. They go about their daily lives in gleaming modern cities with convenient access to professional clinical care. Some may worry about dengue fever, and an unlucky few will actually contract it. Others will be more anxious about threats like MERS-CoV or particular strains of influenza that are much less common than dengue, but with much higher fatality rates. There are no vaccines or cures for these viral infections. Malaria, by comparison, is not only thought of as a distant threat, but is also widely believed to be completely preventable and curable with inexpensive simple therapies. This is an illusion borne of a well-to-do urban worldview. In truth, the Asia-Pacific region is rife with endemic malaria and it faces challenges in mitigating and eliminating this serious problem.
The challenges are steep. There is no vaccine against malaria. Emerging strains of drug-resistant malaria threaten incurable infections. Some infections cannot be treated safely and patients suffer repeated clinical attacks over many months. Other infections derive from forest-dwelling monkeys. About two billion throughout the Asia Pacific live at risk of the infection and tens of millions contract it each year.1 Unknown numbers, perhaps as many as two hundred thousand each year, do not survive the malaria attack.2 This article explores the Asia-Pacific malaria problem and the misplaced broad public complacency regarding it.
The highest risk in urban centers is not malaria itself, but ignorance of or indifference to the malaria occurring in rural areas. The educated, empowered and endowed sectors of Asia-Pacific metropolises can act against malaria in the region if they see and understand the formidable problem and the challenges faced in eliminating it from the region. This article aims at such awareness.
What is Malaria?
Malaria is a term that encompasses a wide variety of diseases caused by single-celled parasites in the genus Plasmodium. There are over 170 species in this genus that infect particular species of mammals, birds and reptiles. Only 5 species are known to routinely infect humans: Plasmodium falciparum, Plasmodium vivax, Plasmodium malariae, Plasmodium ovale, and Plasmodium knowlesi. Among these, P. falciparum and P. vivax cause the vast majority of infections. All of these parasites follow a complicated life cycle that depends upon particular species of mosquitoes in the genus Anopheles. The ability to transmit malaria by these species varies among them like the ability to play chess among humans – from those who don’t know how to grand masters. While it is true that mosquitoes carry malaria from one person to another, in a strictly biological sense the parasites use humans to carry malaria from one mosquito to another – the plasmodia have sex in the mosquito, which makes it, and not us, the definitive host for these parasites. Figure 1 illustrates the life cycle of P. vivax, which is only slightly different from the other species, but in an important way to be explained later in this article.
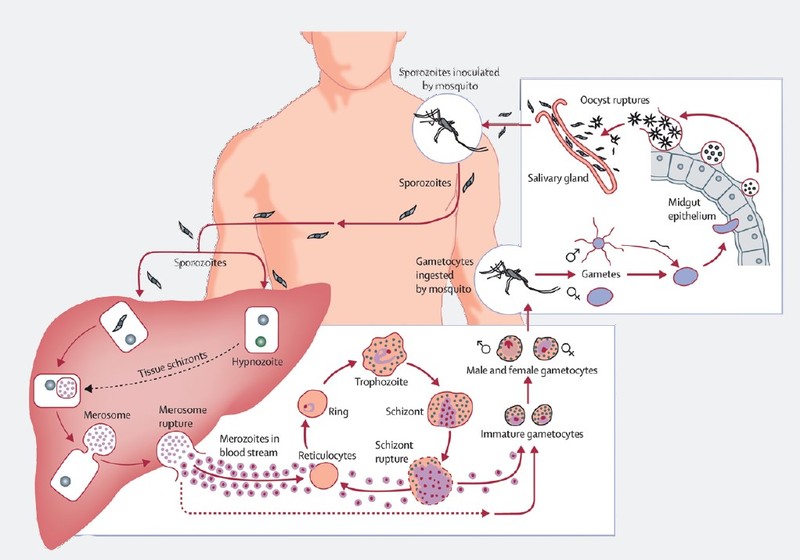
Figure 1. The extraordinary complexity in the |
About a week or so after being bitten and infected, people begin to show symptoms as parasites emerge from the liver and begin infecting red blood cells. The invasion, rupture and reinvasion of red blood cells account for the cyclical nature of the intense fever and chills of a malaria attack. If the infection is not properly diagnosed, or the patient waits too long before seeking treatment, the infection can progress to death in people who lack a partial immunity by prior chronic exposure to malaria. This is true of all of the species of malaria, but especially P. falciparum, P. knowlesi, and P. vivax. Even with prompt diagnosis and appropriate treatment, these infections (excepting P. malariae) lead to intense illness with complete debilitation for at least several days. It is a devastating illness and fatal if not properly managed. The causes of death by malaria are many, including coma, severe anemia, respiratory distress, liver or kidney failure, and shock.
One of the primary reasons malaria tends to be almost invisible is its affinity for impoverished and isolated rural areas, and its aversion to urban environments. Access to quality healthcare in cities bodes poorly for parasite survival. Further, the anopheline mosquito vectors do not survive in urban environments and are not found there. The single known exception to this rule is a particular species, Anopheles stephensi, which thrives in the massive cities of India and causes a great deal of malaria in them. That species adapted to breeding in sunlit pools of clean rooftop water created by air conditioning units. Most mosquito vector species, however, have no tolerance of urban grime. Malaria victimizes the poorest of the poor in rural settings, those having limited access to rudimentary health care that governments struggle to deliver to the many remote peripheries of modern civilization. These people are among the most invisible to us, and they suffer tremendously in vast numbers from malaria and other diseases endemic to the Asia-Pacific.
Malarious Asia-Pacific
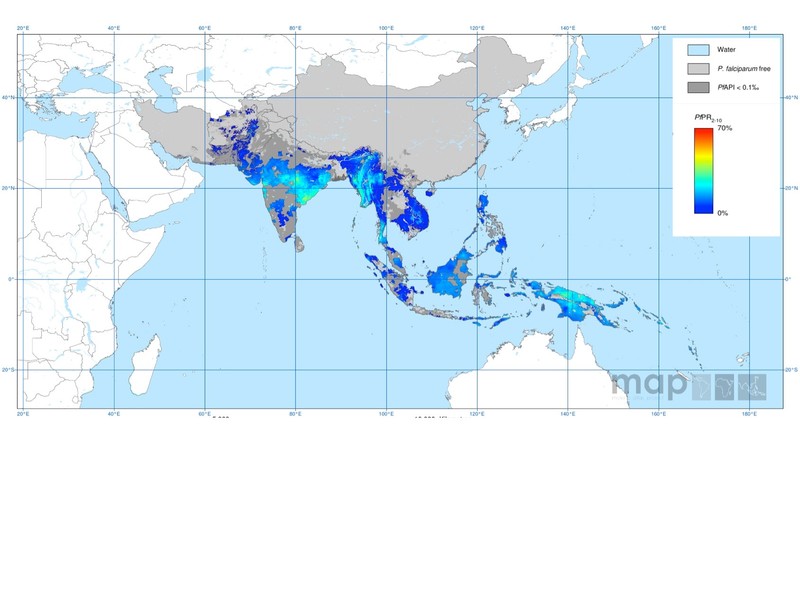
A glance at a world map of the levels of malaria prevalence reveals what most residents of the Asia-Pacific do not realize – that malaria is not solely an African problem, it is all around us right here in the region, and quite a lot of it. The two maps of Figure 2 show the distribution of the two dominant species of parasites that cause malaria, P. falciparum and P. vivax. Wherever there is color, even if blue, indicates stable transmission of malaria, meaning it is almost always present. The dark grey areas indicate unstable transmission, where malaria is only sometimes present. Figure 3 zooms in on the Asia-Pacific and reveals the extraordinary patchwork of transmission, both broad swaths of persistent stable transmission along with a scattering of both very high risk and risk-free pockets.

|
 |
| Figure 2. Maps showing the distribution of malaria risk globally for Plasmodium falciparum (top) and Plasmodium vivax (bottom). See color keys in Figure 3. Courtesy of the Malaria Atlas Project, University of Oxford, United Kingdom. | |
Notice that the distribution of P. vivax reaches much farther north than P. falciparum. There are a couple of important reasons for this. First, this species develops quicker at lower ambient temperatures in its cold-blooded mosquito host, allowing it to thrive in temperatures P. falciparum cannot tolerate. Secondly, P. vivax is able to place dormant forms in the human liver (called hypnozoites, see Fig.1), providing it a safe haven during the harsh winters on the Korean Peninsula, for example, when there can be no mosquitoes to transmit them.
 |
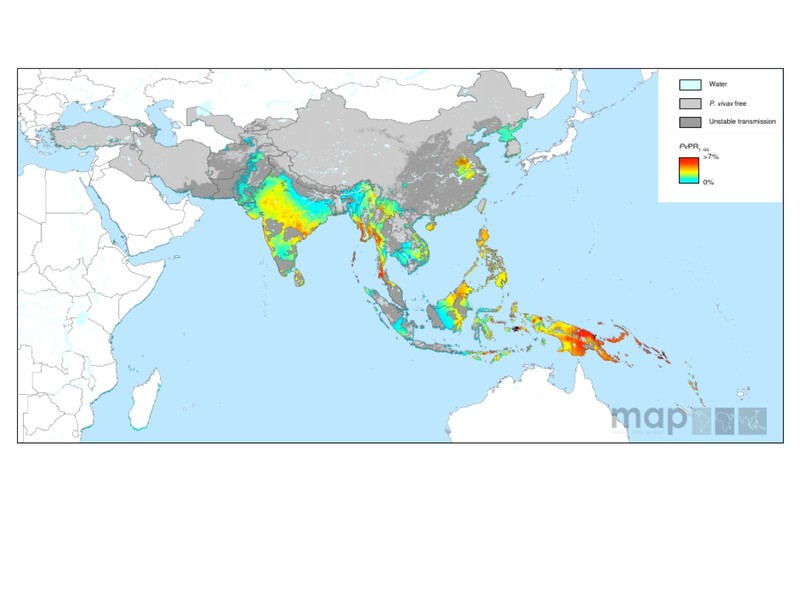 |
| Figure 3. Maps showing the distribution of malaria risk in the Asia Pacific for Plasmodium falciparum (top) and Plasmodium vivax(bottom). “PR” indicates prevalence rate, or the percentage of residents found infected by malaria parasites in population surveys of blood by microscopic examination. The scales between P. falciparum and P. vivax differ for biological and epidemiological reasons. Courtesy of the Malaria Atlas Project, University of Oxford, United Kingdom. | |
The World Health Organization monitors malaria reporting globally, and in 2013 it estimated a total of 11.2 million cases of P. vivax in the Asia-Pacific, along with 25 million cases of P. falciparum.4 That’s 36.1 million attacks of malaria in the region. Some scientists believe these WHO estimates are underestimated by a large degree.5 Remarkably, in the instance of P. vivax, over 80% of all attacks globally occur in the Asia-Pacific, making this principally a regional problem.
Malaria Problems of the Asia Pacific
Malaria as a public health problem varies tremendously around the globe with respect to difficulties faced in striving to solve it. Malariologists in Africa wrestle with very different technical issues from those managed by malariologists in the Asia-Pacific. It is important to understand that technical progress and health dividends in Africa will not necessarily translate to the same in the Asia-Pacific. A brief exploration of three malaria problems unique to the region will serve to emphasize that important point: artemisinin-resistant P. falciparum, primaquine therapy against P. vivax, and monkey malaria. The challenge in Africa is a very heavy burden of infection by a single species of parasite P. falciparum, which until today remains sensitive to the frontline drugs against it. The species P. vivax is virtually absent from most of Africa, as are the malarias transmitted from monkeys or apes to humans.
Artemisinin-resistant P. falciparum
Forty years ago the drug chloroquine served as the primary treatment for all malarias worldwide. The extraordinary history of the development of this workhorse drug includes Nazi agents in Algiers and Allied capture of an experimental formulation of the drug in 1943.6 Licensed in the USA in 1946, its useful life began to unravel at the border between Thailand and Cambodia in the 1960s. The parasite P. falciparum evolved a means of surviving chloroquine, and with continued use the resistant strains overwhelmed and dominated the sensitive strains. Over the ensuing 20 years, those resistant strains spread around the globe. Millions are thought to have lost their lives to infections by resistant strains treated with what had become a useless drug.7 Eventually, after a great deal of research and advocacy for change, chloroquine was replaced with a new class of drugs called the artemisinins – discovered by a medical science unit of the Chinese Army working in support of the North Vietnamese during the war with the Americans (by the 2015 Nobel laureate Dr. Y. Tu).8 That warfare drives critical advances in malaria therapy that cease in peacetime is a sad testament to its low priority when it is only attacking and killing civilians. This is changing, however. In 1999, the Medicines for Malaria Venture at Geneva was created for taking up the important business of discovering, evaluating and licensing medications affordable to the poor who are most affected by malaria. They have made great strides with generous support from sponsors and donors.9
The artemisinin combined therapies (ACTs, artemisinin plus a partner drug) today comprise the frontline against sickness and death caused by malaria. Thanks to their broad implementation, along with many preventive measures like mosquito nets and practical diagnostics for malaria, global mortality due to malaria has fallen by half since 2000.10 Unfortunately, the drug resistance drama that played out in western Cambodia with chloroquine fifty years ago, is today repeating itself – resistance to ACTs was detected in the same area in 2008 and has since spread much wider (Figure 4). No one understands exactly why, but western Cambodia seems to be a cradle of drug resistant malaria. It seems likely that the decades-long unregulated use of artemisinin alone during the strife and warfare in Cambodia, without the partner drug of ACTs (which is there in order to delay onset of resistance) selected for those resistant mutants. The threat of this menace causing a surge in malaria mortality is not mere hyperbole – it is real because we have no practical therapeutic options in our global malaria medical kit. The specter of untreatable falciparum malaria looms over the globe, and it is an Asian-Pacific responsibility to manage the problem.
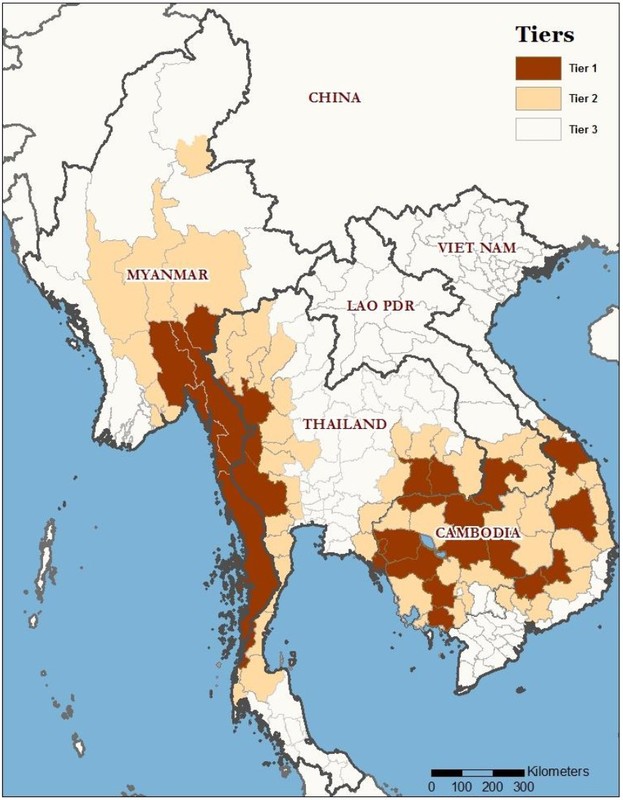
Figure 4. Map illustrates penetration of (2, yellow), absent (3, white). |
Primaquine Therapy of P. vivax Malaria
As explained, P. vivax places dormant forms in the human liver that can cause repeated clinical attacks up to about 2 or 3 years after a single infectious bite by a mosquito.
The only drug that kills these dormant forms is called primaquine – another product of World War II, the Asia-Pacific War in particular.11 The Dutch on Java in 1941 produced over 95% of the world’s supply of quinine, and when the Allies lost access to that supply they turned to synthetic drugs. One of those caused the only therapy against dormant liver stages to become especially toxic.
The US Army then launched a search for a new drug in 1943, and in 1952 primaquine was licensed for this use.
In many respects, primaquine is woefully inadequate as a drug. Its many problems are rooted in its toxicity to people with an inherited blood disorder called glucose-6-phosphate dehydrogenase (G6PD) deficiency. People having that disorder lead healthy lives of normal longevity, but become seriously ill when exposed to specific drugs that destroy their red blood cells.
Primaquine is one of those drugs, and the doses needed for treating P. vivax can cause death in the most severe types of G6PD deficiency.
Unhappily, G6PD deficiency is a highly prevalent human genetic disorder (typically about 8% of people in malaria-endemic nations), impacting 400 million people globally, most of them living in the Asia-Pacific (Figure 5).
Even worse, the most severe types of G6PD deficiency dominate those found in the Asia-Pacific.12
The diagnosis of G6PD deficiency is relatively simple in a laboratory setting. If accomplished, the G6PD normal majority enjoys the enormous clinical benefit of primaquine therapy without risk of harm. However, in the impoverished rural tropics where the vast majority of malaria patients live, such services are almost universally absent. Recent work vigorously strives to address this serious problem that denies most patients with P. vivax access to safe primaquine therapy.13
Another unfortunate fact is the strains of P. vivax occurring in the Asia- Pacific are among the most aggressive with respect to how frequently and often they will cause repeated attacks from the dormant liver stages. Scientists and doctors long thought P. vivax infection to be inherently benign and not threatening, but over the past decade studies at hospitals in rural areas revealed it as very often associated with severe illness and death.14 It is perhaps likely that most of those poor outcomes derive from the repeated multiple attacks from the untreated liver forms of the parasite. In the absence of G6PD diagnostics, care providers must choose between risk of serious harm caused by primaquine, or harm caused by the infection by withholding the treatment.
Monkey Malaria
Another problem of malaria unique to the Asia-Pacific is infection by P. knowlesi. This species is very different from the other four species infecting humans because we are not its natural host. Humans acquire P. knowlesi in forests inhabited by macaques, the animal that P. knowlesi naturally infects. The first known report of human infection by this species appeared in 1965 – in an American CIA agent working at night in the forests of peninsular Malaysia.15 He returned to Washington where he was correctly diagnosed only in a most extraordinary series of coincidences worthy of CIA intrigue. This lone infection for decades was considered a one-off event and it was widely believed that P. knowlesi did not routinely infect humans.
In 2004, Malaysian scientist Balbir Singh and his colleagues at the University of Malaya at Sarawak unveiled a serious threat from this species.16 Not only was P. knowlesi infecting humans, but it was doing so often and ending in death for many.17 The infection had been diagnosed as P. malariae (which it closely resembles under the microscope). However, true P. malariae malaria is usually relatively benign (although chronic infections can cause irreversible and ultimately fatal kidney failure). Patients were coming in with what seemed to be that species but with very aggressive infections and acute disease states. Professor Singh and his team solved the mystery. Today we know that most of the malaria that occurs on Malaysian Borneo is in fact P. knowlesi. A map of the areas of known risk of P. knowlesi infection reveals it to be uniquely Asian-Pacific (Figure 6).

Figure 6. Map illustrates relative likelihood of |
Eliminate Malaria!
Beginning about a decade ago, momentum began building to mobilize resources to eliminate malaria transmission, leading ultimately to its eradication as a human health problem.18. Taking the personal encouragement and example of Bill & Melinda Gates expressing malaria elimination as a vision, WHO Director General Margaret Chan announced in 2008 that WHO would embark on a global malaria control strategy that aimed to eliminate malaria. This represented a fundamental paradigm shift of strategy and tactics in malaria control as a public health endeavor. Deliberately and aggressively attacking malaria where it was not highly prevalent, or striving to interrupt transmission where it was highly prevalent, had long been viewed as impractical and even dangerous.19The danger lies in failure. During the 1950s and 1960s the WHO (largely spurred by the US State Department and US funding) undertook the Global Malaria Eradication Program (GMEP).20 Huge strides were made in reducing malaria, especially in the Asia-Pacific. However, in 1969 the WHO abandoned the campaign, leaving behind malaria control programs that were no longer functional. Further, research on malaria effectively ceased after the program commenced due to optimism regarding successful global eradication. Between 1970 and 2000 global burdens of malaria morbidity and mortality surged powerfully due to technical, material, and personnel deficiencies spurred by the GMEP. Elimination strategy invites risk of rebounds of malaria in the wake of failure.
The year 2030 is the declared goal for the elimination of malaria transmission across the Asia-Pacific. In 2008 malaria technical experts formed the Asia Pacific Malaria Elimination Network that draws them together with the national malaria control programs of 18 nations with declared malaria elimination goals. They aimed to support those programs in shifting from control to elimination strategy and tactics where deemed feasible. Mobilizing political and fiscal support and momentum, the Asia Pacific Leader’s Malaria Alliance was created in 2013 by the heads of national governments in the region. The risks of powerful rebounds of malaria with failure to achieve real elimination are soberly acknowledged and impel the urgency of full commitment to the task.
The problems with malaria in the Asia-Pacific summarized here will challenge elimination goals. Each of those three major challenges requires solutions unique to the malaria of this region. Acknowledging these as problems of the Asia-Pacific appropriately focuses regional attention, enthusiasm, and resources for attacking them vigorously. The temptation to passively wait for others in distant regions to deal with their own unique malaria problems to pass along the technical fruit of their labors must be resisted. They cannot deliver the goods the Asia-Pacific requires. These are our problems to solve.
Recommended citation: J. Kevin Baird, “Malaria in the Asia-Pacific Region”, The Asia-Pacific Journal, Vol. 13, Issue 44, No.1, November 9, 2015.
J. Kevin Baird served for 22 years on active duty in the US Navy Medical Service Corps as a malaria specialist, principally in the Asia-Pacific, retiring in 2006 with the rank of Captain. He is currently Professor of Malariology at the Centre for Tropical Medicine, Nuffield Department of Medicine, Oxford University and directs the Eijkman-Oxford Clinical Research Unit on behalf of that university and the Eijkman Institute for Molecular Biology in Jakarta, Indonesia. Prof. Baird has resided in Indonesia for over 20 years and is co-author of the book War Crimes in Japan-Occupied Indonesia: A Case of Murder by Medicine, Potomac Books 2015, with Sangkot Marzuki, former director of the Eijkman Institute and current President of the Indonesian Academy of Science.
•Vivian Blaxell, Yellow Blood: Hepatitis C and the Modernist Settlement in Japan
References
1 World Health Organization. World Malaria Report 2014. Geneva.
2 Hay SI, Gething PW, Snow RW. India’s invisible malaria burden. Lancet 2010; 376: 1716-17.
3 Mueller I, et al. Key gaps in the knowledge of Plasmodium vivax, a neglected human malaria parasite. Lancet Infectious Diseases 2009; 9: 555-66.
4 Ibid, WHO
5 Ibid, Hay SI, Gething PW, Snow RW
6 Coatney GR. Pitfalls in a discovery: the chronicle of chloroquine. American Journal of Tropical Medicine and Hygiene 1963; 12: 121-8.
7 Attaran A, et al. WHO, the Global Fund, and medical malpractice in malaria treatment. Lancet 2004; 363: 237-40.
8 Tu Y. The discovery of artemisinin (qinghaosu) and gifts from Chinese medicine. Nature Medicine 2011; 17: 1217-20.
10 Murray CJ, et al. Global, regional and national incidence of mortality for HIV, tuberculosis, and malaria during 1990-2013. Lancet 2014; 384: 1005-70.
11 Baird JK. Resistance to therapies for infection by Plasmodium vivax. Clinical Microbiology Reviews 2009; 22: 508-34.
12 Howes RE, et al. G6PD deficiency prevalence and estimates of affected populations in malaria endemic nations: a geostatistical model-based map. Public Library of Science Medicine 2012; 9: e1001339.
13 World Health Organization. Control and elimination of Plasmodium vivax malaria: a technical brief. Geneva. 2015.
14 Baird JK. Evidence and implications of mortality with acute Plasmodium vivax malaria. Clinical Microbiology Reviews 2013; 26: 36-57.
15 Baird JK. Malaria zoonoses. Travel Medicine Infectious Diseases 2009; 8: e2780.
16 Singh B, et al. A large focus of naturally acquired Plasmodium knowlesi infections in human beings. Lancet 2004; 363: 1017-24.
17 Cox-Singh J, et al. Plasmodium knowlesi in humans is widely distributed and potentially life threatening. Clinical Infectious Diseases 2008; 46: 165-71.
18 Malaria: control vs elimination vs eradication. Lancet 2011; 378: 1117.
20 Baird JK. Resurgent malaria at the millennium: control strategies in crisis. Drugs 2000; 59: 719-43.