

By The Weston A. Price Foundation
Blood is the essence of life. It is useful to examine the blood under a microscope to look for any changes in reaction to a stressor. In this exploratory study, ten human subjects were exposed to a cell phone radiation stressor. Their blood was examined under a dark-field microscope to look for changes, if any, from the cell phone microwave frequency. We also investigated whether there might be a protective effect on the blood from consuming the recommended Weston A. Price Foundation (WAPF) diet.
The world has rapidly changed over the past few decades with the advent of cell phones. Almost seven billion cell phones are now used worldwide, of which over five billion are in developing countries. As of January 2014, 90 percent of American adults possessed cell phones, and 58 percent of the users had smart phones.1 Due to increasing affordability along with the many useful functions that cell phones provide, the explosion in cell phone usage is not surprising. Indeed, they have become the leading technology in the brave new wireless world of communications.
The Safety Controversy
Are cell phones completely safe? There is no consensus on how to address this question with its various complex, multifaceted issues. There are many factors to consider, such as the duration of exposure, a person’s age, whether the radiation dose is cumulative or not, the long-term use over a person’s lifetime, pregnancy, and how cell phones are being used—and stored—on the body.
Cell phones and smart phones are powered by microwaves, part of the electromagnetic spectrum, which range from 300 to 3,000 megahertz (MHz). The key frequencies used in cell phone communications worldwide are 850, 900, 1,800, and 1,900 MHz (1.9 gigaHz). (A microwave oven, which heats water and the water in food, works on 2450 MHz.)
Cell phones and smart phones both receive and emit these frequencies, smart phones emitting far more than the old clam-shell type of cell phone. The radiation they receive comes from cell phone towers, which is ambient, meaning that it is everywhere, and we are all receiving it, all the time. The radiation coming out of the smart phone is of much higher intensity than that coming from cell phone towers, unless one happens to be located very close to a tower.
There are guidelines in the U.S. for short term exposure to cell phone frequency microwaves, defined in terms of the Specific Absorption Rate (SAR), the rate at which energy is absorbed by the human body when exposed to radio frequency radiation. Specifically, the Federal Communications Commission (FCC) in the United States requires that phones sold have a SAR level at or below 1.6 watts per kilogram (W/kg) taken over the volume containing a mass of one gram of tissue that is absorbing the most signal.2 This is a guideline, not a standard, and is solely based on heat generation by cell phone microwaves, because microwaves are well known to produce tissue heating. However, besides heating, there are other types of biological effects from the extremely low-level microwaves associated with cell phones, called “nonthermal” effects. The Russians have conducted many studies on the nonthermal effects, which they consider more significant than thermal effects, and as a result, they adopted a more stringent guideline that is sixty to one hundred times lower than U.S. guidelines.
Studies on the nonthermal biological effects of microwaves have taken place mostly outside of the U.S., on animals, cell cultures, and humans, for the past several decades. This research has found effects at every level of organization of life, from the behavior and performance of humans and animals down to the molecular and genetic levels. Studies show effects on the brain, stem cells, reproductive organs, enzyme activities, and sperm quantity and quality in animals and humans. More specifically, changes in calcium transport from cells, altered enzyme activities, increased cell proliferation of human epithelial cells, increase in breaks in DNA in animal cells, changes in brain blood flow in healthy people, leakage of proteins through the blood brain barrier, and decreased sperm count and motility are some changes that have been documented. Two recent reviews on nonthermal effects summarize the findings from over two hundred scientific papers.3,4 Many of these nonthermal effects are considered controversial because they have not been replicated by other researchers or published in what are considered to be the top peer-reviewed journals. There is also the paradox that lower intensity microwaves sometimes produce larger biological effects than higher intensities, known as the biological “window” effect. The physical mechanisms of how low-level microwaves can cause so many different biological effects are not well understood. There is no unifying theory that combines the many reported biological effects of low-level microwaves to explain the possible health risks of cell phone radiation exposure.
Most of the studies on cell phone radiation and its biological effects are short-term exposure studies. But some epidemiological studies suggest that chronic exposure to low-level microwaves may increase the risk for cancer and other tumors. In fact, the World Health Organization’s (WHO) International Agency for Research on Cancer (IARC) has classified radio frequency electromagnetic fields as possibly carcinogenic to humans based on an increased risk for glioma, a malignant type of brain cancer, and acoustic neuroma, a benign tumor in the ear area, both associated with wireless phone use.5 However, given the potential twenty-to-thirty year latency period of cancer development, the effect of cell phone radiation on cancer risk as well as the risk for other chronic health problems may not be fully understood for many years to come.
Exposure to various electronic devices including cell phones, cell phone towers, DECT (digitally enhanced cordless telecommunications) and other cordless phones, and wireless modems has been found to cause a variety of symptoms in some people, including headaches, anxiety and irritability, restlessness, sleep problems, difficulty in concentration, ringing in the ears, heart palpitations and fatigue. This is labeled Electro-Hypersensitivity Syndrome (EHS). In 2011, WHO estimated that 3-6 percent of the world population suffered from EHS. It is possible that the percentage may grow as chronic exposure to Wi-Fi continues.
Most studies on cell phone radiation have tested cell cultures and animals rather than humans. No formal studies examining the blood of humans exposed to cell phones have been found in the medical literature to date. A small number of studies on human lymphocytes showing changes in cell nuclei and impaired DNA repair have been published. In the present study, we investigated only short-term effects of cell phone radiation exposure on normal healthy persons.
Research Questions
1. Does the blood as observed under a darkfield microscope change after human subjects are exposed to a smart phone for a short time period?
2. Does eating a mostly WAPF-recommended diet help protect the blood from the effects of cell phone radiation?
Research Design
An exploratory pilot study with ten normal healthy adult subjects who consumed the WAPF-recommended diet to varying degrees was conducted to look for an effect. This study is an outcome type of design in which each subject served as his or her own control. A technique that has been called live blood analysis or whole blood microscopy was used. Peripheral blood samples taken from subjects before and after different types of exposure to a cell phone were placed under a microscope, photographed, scored by a trained researcher using a Likert scale, and compared. These data were analyzed to discover which of various blood factors may have changed in relation to exposure condition, diet, subject age, and personal history of cell phone use. Because the sample size (N=10 subjects) was very small, statistical tests were not done.
Subjects
Prospective subjects were recruited from the WAPF email list in the San Francisco Bay Area. Responders completed a background questionnaire to see whether they qualified. Qualified subjects were normal healthy adults with no chronic disorders or conditions and who consumed the WAPF diet to varying degrees. No prior use of a cell phone was required. Subjects who fully participated consisted of two males and eight females ranging from twenty-seven to seventy-five years of age, with a mean age of 53.3 years. Their daily consumption of the WAPF diet ranged from 20 to 98 percent, with a range from two to twenty years on the diet, and an average of 6.1 years on the diet. Eight of the ten subjects possessed a cell phone, of whom six had a smart phone. The average number of years that the subjects had used a cell phone was 10.8 years. Cell phone use among them varied from none whatsoever to twenty years of daily use, and with usage up to 3.5 hours per day. Subjects spent an average of 1.2 hours per day using a cell phone. One subject claimed some sensitivity to electrosmog, although she had not been formally diagnosed with EHS and did not complain of any symptoms during the trial.
Subjects completed a questionnaire about their health, diet and personal cell phone habits. Written informed consent was given by those who participated in the study. Each subject received a modest fee for participating in a three-hour experimental session.
Methods and Procedures
Live blood analysis involves examination of a small droplet of fresh capillary blood typically taken from the fingertip. This is observed under an optical microscope at magnifications from 600 to 1200x. A camera mounted on the microscope records digital photographs of the blood samples. This technique provides information on the ecology of the blood, sometimes referred to as the “biological terrain.” Live blood analysis has traditionally been used in clinical medicine to look for the presence of certain parasites including the malaria organism and the spiral-shaped bacteria that causes Lyme disease. It is a research tool sometimes also used in holistic health assessment. The size, shape, variability, and cellular integrity of the red blood cells (RBCs) can readily be seen, as well as any stickiness and aggregation of the RBCs. The presence and relative number of white blood cells and their subtypes are noted, along with the motility (movement) of these cells. The blood plasma is checked for platelet aggregates, the formation of fibrin, the presence of microbial and parasitic forms, as well as particulates including cholesterol, crystals, and various contaminants.
This study utilized a custom-built, dark-field microscope attached to a digital video camera system with zoom lens linked to a computer monitor. Software was used to capture and store microphotographs for subsequent analysis. The blood specimen was lit by means of light delivered through fiber optics attached to the microscope condenser to prevent sample heating. A sterile lancet was used to collect a droplet of peripheral blood from the fingertip, which was immediately placed on a glass microscope slide and covered with a glass cover slip. Oil immersion lenses at the microscope objective and dark-field condenser were used for image optimization.
A microphotograph of normal healthy blood from a person consuming the WAPF diet is shown in Figure 1. This photograph shows the blood immediately after it is drawn. Round RBCs appear uniform in size, separated from one another, and with no debris in the blood plasma.
Subjects fasted for at least five hours and refrained from exposure to cell phones for four hours prior to individual appointments in the study. During their three-hour experimental session, subjects were allowed to drink only water. Each subject was given three blood tests associated with three different exposure conditions as described below. Each blood sample was evaluated and scored for different blood factors. These factors include the shape of red blood cells and membrane distortion; state of aggregation of the red blood cells, including clumping, rouleaux formation (cells stuck together in rolls) and stickiness; white blood cell shape and motility; and the degree of early clotting factors including platelet aggregates and presence of fibrin. A Likert scale from 0 to 6 was used to score the blood factors, in which 0 indicates an absence of the blood factor, and larger numbers indicate greater levels of the blood factors observed in the blood samples. This method has been previously described in detail in other studies on diet reported in this journal.6,7
Three blood tests were performed on each subject as follows: (1) initially, prior to cell phone exposure (baseline condition); (2) following exposure to a smart phone in receiving mode placed in a backpack worn by the subject for 45 minutes (carrying condition); and (3) following active use of the cell phone for 45 minutes (active use condition). These are the two conditions in which most people use a cell phone. Cell phones can also be put in “airplane mode,” in the sense that the user cannot make a call or access the web. However, the phone is still in communication with the nearest cell phone tower.
Ten or more typical blood microphotographs were made for each of the three exposure conditions. During the active use condition, the subjects continually used the cell phone’s communication functions to access the Internet and to make phone calls. Also in the active use condition, subjects placed the cell phone near their heads at least twice for approximately five minutes each time during phone calls. During other times while making phone calls, subjects used the speaker phone mode while holding the phone in one or both hands. Following photographic analysis of all blood testing, the Likert scale data were analyzed to see which factors—diet, age, and personal cell phone habits—correlated with any observed blood changes.
The cell phone used for subject exposure was a particular model of a smart phone, and the same network carrier was used throughout the study. (Brand and model number of smart phone and network provider used in the study are deliberately withheld from this report.) Subjects remained in the laboratory throughout the experimental sessions. The exposure times and phone call durations for subjects were timed and otherwise controlled such that the cell phone radiation exposure for each subject was the same as possible for each condition. The ambient power level of radiowaves (including microwaves) in the laboratory, as measured by a radio frequency meter, was typically -45dBm corresponding to a power density of 18 microWatts per square meter. No other devices were present that could be significant sources of microwaves.
Results
The baseline blood tests of all subjects revealed normal healthy blood in almost all cases as has been reported previously for those consuming the WAPF-recommended diet.6 Figure 2 shows a photograph of normal healthy blood from a female subject, seventy-five years old, in baseline condition. The red blood cells (RBCs) are mostly circular, although they appear to be slightly sticky as some cells overlap, and the plasma is relatively clear.
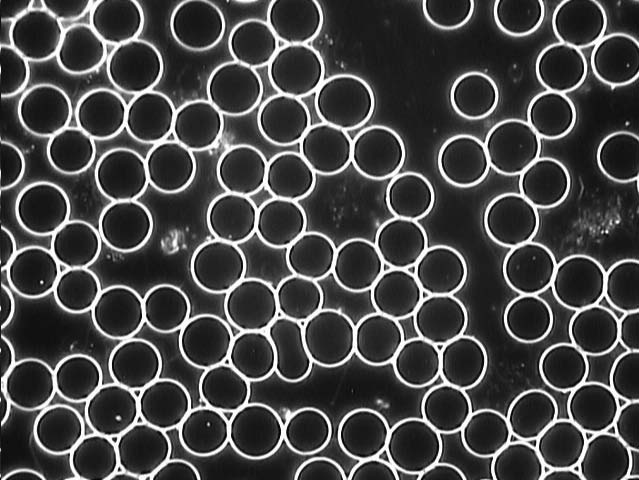 Figure 1: Healthy blood showing round, separate RBCs and clean blood plasma.
Figure 1: Healthy blood showing round, separate RBCs and clean blood plasma.
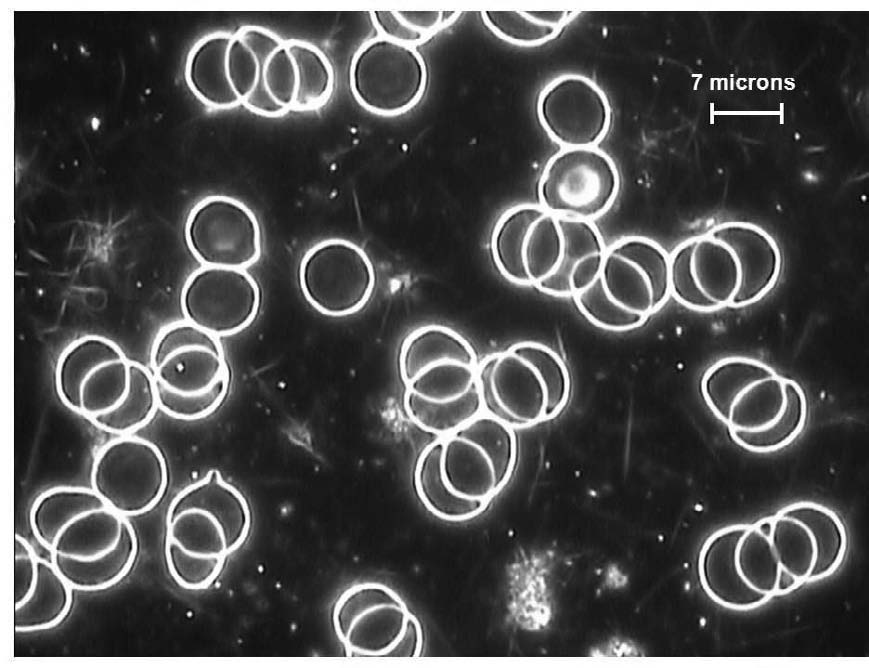 Figure 2: Baseline condition showing normal, healthy blood from 75-year-old female subject.
Figure 2: Baseline condition showing normal, healthy blood from 75-year-old female subject.
Figure 3 shows the blood from the same female immediately after the carrying condition. The RBCs are entirely stuck together in rouleauxtype aggregates, which look like rolls of coins.
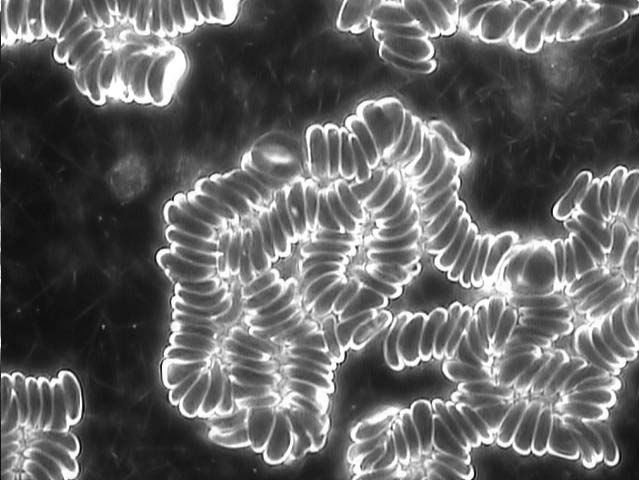 Figure 3: Carrying condition of 75-year-old female subject showing all RBCs in rouleaux.
Figure 3: Carrying condition of 75-year-old female subject showing all RBCs in rouleaux.
Figure 4 shows the blood from the same female 45 minutes later after using the cell phone in active communication mode. The rouleaux have dissipated, although the RBCs are still aggregated. Most RBCs are misshapen rather than round. Many RBCs show spiky projections on the surface, which are abnormal, spiculed RBCs called echinocytes. This particular subject, seventy-five years old and the oldest person in the study, showed the most characteristic changes in the blood following both exposure conditions.
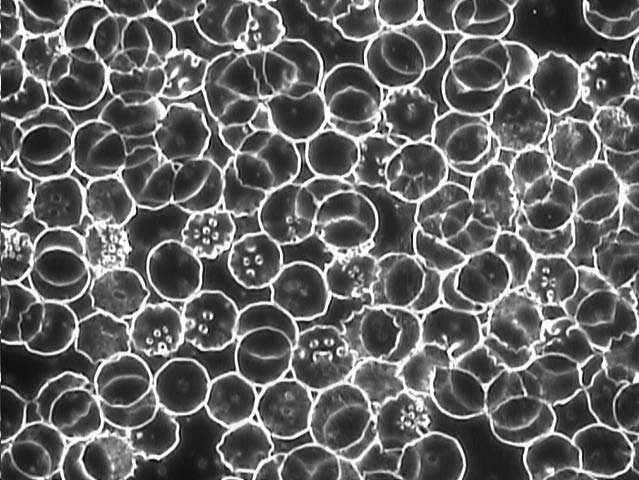 Figure 4: Active use condition of same subject showing most RBCs are misshapen.
Figure 4: Active use condition of same subject showing most RBCs are misshapen.
Most of the other subjects showed similar but less clear-cut effects. As another example, Figure 5 shows the blood from a male, age fifty-five, in baseline condition. The red blood cells (RBCs) are mostly round and separate, and the plasma is relatively clear.
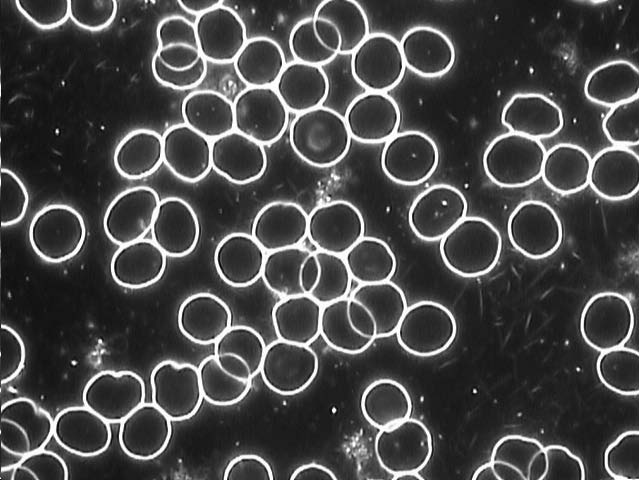 Figure 5: Baseline condition of male, age 55, showing normal, healthy blood.
Figure 5: Baseline condition of male, age 55, showing normal, healthy blood.
Figure 6 shows the blood from the same male subject immediately following the carrying condition. The red blood cells are observed to be loosely aggregated. Some of the cells are no longer round but misshapen.
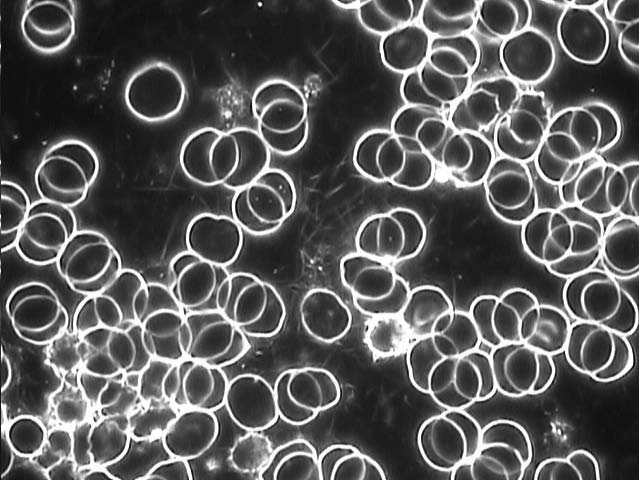 Figure 6: Carrying condition of same male showing aggregated cells and a few misshapen RBCs.
Figure 6: Carrying condition of same male showing aggregated cells and a few misshapen RBCs.
Figure 7 shows the blood from the same male subject immediately following the active use condition. Every RBC appears to be misshapen. Many of the cells show spikes and are echinocytes.
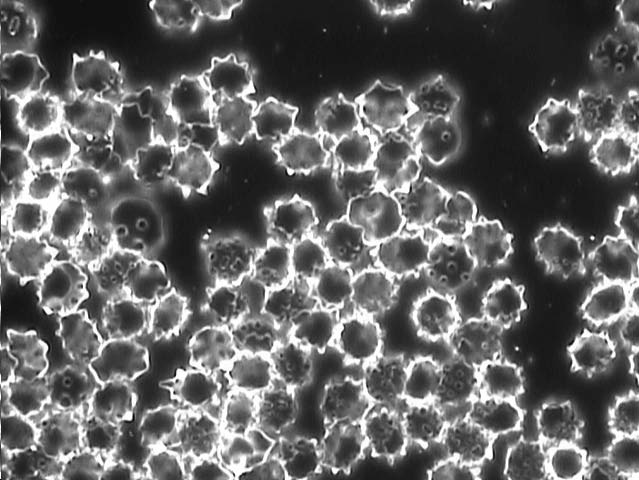 Figure 7: Active use condition of same male subject showing all RBCs are misshapen.
Figure 7: Active use condition of same male subject showing all RBCs are misshapen.
Because subjects were holding the phone during the active use condition, their fingers received considerable microwave radiation doses. So we compared peripheral blood drawn from the fingertip as well as from the toe of one female subject, age fifty-five, in the active use condition to determine whether the blood changes were localized or not; see Figures 8 and 9. No difference between fingertip and toe blood was observed.
 Figure 8: Active use condition of female subject, age 55, fingertip blood showing RBCs in rouleaux.
Figure 8: Active use condition of female subject, age 55, fingertip blood showing RBCs in rouleaux.
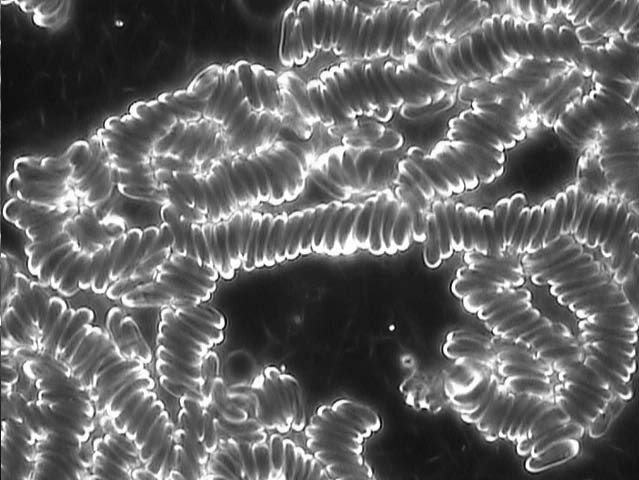 Figure 9: Active use condition of same female subject, toe blood showing RBCs in rouleaux.
Figure 9: Active use condition of same female subject, toe blood showing RBCs in rouleaux.
Nine out of ten subjects showed observable blood changes due to cell phone radiation exposure. One female subject, age fifty-three, did not show a significant effect from exposure in the study. In general, a particular sequence of blood changes was observed for cell phone radiation exposure in which the subjects’ RBCs first became sticky and aggregated, and upon further exposure, for most subjects, the cells became misshapen. We observed no distinct change in other blood factors including platelet aggregation, fibrin, white blood cell morphology and white blood cell motility.
Diet and Blood cell changes
To address the question of whether a higher percentage of WAPF diet served to protect subjects from blood changes, the Likert scale scores of the blood factors were grouped together as follows. Baseline scores were subtracted from the carrying condition scores and also from the active use scores to yield net blood factor changes due to exposure. Then the net scores for rouleaux, other red blood cell aggregates, and protein linkage were summed and called “net RBC aggregates.” The scores for RBC membrane distortions and RBC echinocytes were also added together and called “net RBC shape changes.” Figures 10 and 11, respectively, show the blood scores for the carrying condition and the active phone use condition for each of the ten subjects, arranged in order of percent WAPF diet. In either case, the blood scores for the subjects show no clear correlation with the percent WAPF diets. Thus, it appears that a higher percentage of WAPF diet does not offer protection against observed blood changes following short-term exposure to cell phone radiation.
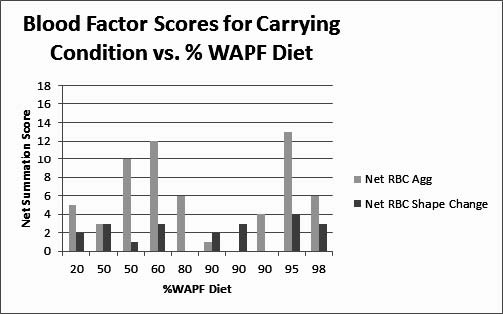
Figure 10. Net blood factor scores for the phone carrying condition show no clear relation to % WAPF diet.

Figure 11. Net blood factor scores for the active use condition show no clear relation to % WAPF diet.
There is a possible relationship between the levels of change observed in the blood with subject age and/or cell phone habits in daily life. Figures 12 and 13 show levels of blood changes observed in subjects immediately following the carrying condition and the active phone use condition, respectively, as a function of subject age. It appears that younger subjects show less aggregated RBCs than older subjects for the carrying condition (Figure 12). It also appears that younger subjects show less aggregated RBCs as well as less blood cell shape changes than older subjects for the active use condition (Figure 13). Figure 14 shows the reported use of cell phone on the average per day for each subject. In general, younger subjects reported using their cell phones a greater number of hours per day than older subjects. Unfortunately, in this small study the distinction between age and cell phone use cannot be separated.
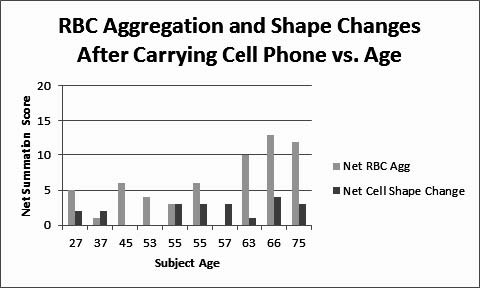
Figure 12. Net blood factor scores in subjects after carrying cell phone vs. subject age.
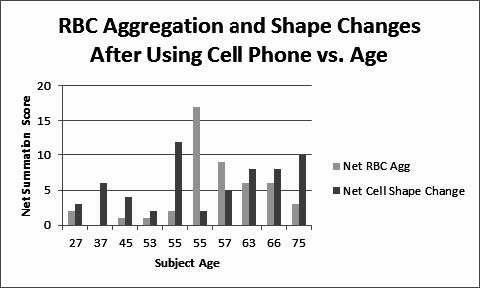
Figure 13. Net blood factor scores in subjects after active use of the cell phone vs. subject age.
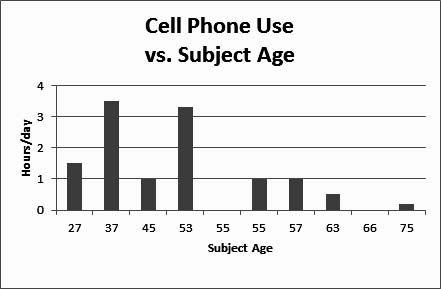
Figure 14. Cell phone habits for each subject as self-reported daily use.
Figure 15 summarizes the overall observed effects on the blood from short-term exposure to cell phone radiation for both the carrying condition and active use condition. The observed changes are substantial in magnitude. For the carrying condition, RBC aggregates dominate, while RBC shape changes are fewer. For the active condition, RBC shape changes dominate, and RBC aggregates, while present, are somewhat less pronounced.
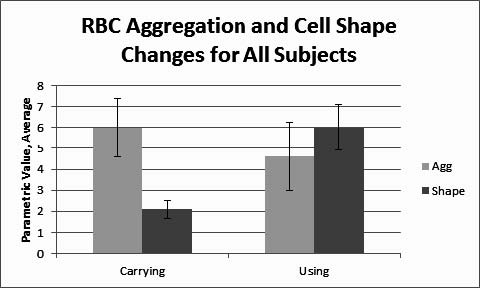
Figure 15. Blood changes observed for the whole group, averaged, for the two exposure conditions: carrying and active use. Error bars indicate standard error.
Conclusions and Discussion
Results show substantial changes in the blood from short-term cell phone radiation exposure in nine out of ten human subjects. RBC aggregation and stickiness were mainly observed following 45 minutes of exposure to a smart phone in receiving mode worn by subjects in a backpack. By contrast, RBC morphological (shape) changes including the formation of echinocytes (spiky cells) were dominant after subjects actively used the phone for an additional 45 minutes. It appears that RBC stickiness with clumping is the first stage of the cell phone radiation effect. Subsequently, the RBC aggregates tend to break apart, and then cell shape changes occur, in which echinocytes and other misshapen cells are observed. Not all subjects showed both types of changes. The difference in net RBC aggregates between the carrying and the active use conditions are not significant for this small sample, as indicated by the overlap in the error bar values in Figure 15. However, the differences in RBC shape changes between the carrying and the active use conditions appear to be significant.
Such blood morphologies—RBC clumping and misshapen cells—are frequently observed in ill persons or those eating less-than-optimal diets.6,7 Echinocyte formation has been associated with aging RBCs and diseases such as cirrhosis of the liver.8 In a study exposing mice to cell phones, clumped RBCs were found after short- term exposure, and abnormal RBC shapes were observed over longer exposure times,9 which is similar to the results observed in this study.
It is possible that the changes in RBC shape that we observed may be related to functional changes in cell membrane permeability. Other studies have reported changes in RBC membranes following exposure to microwaves, too. Low-power microwave radiation increased membrane permeability and destabilized the cell membrane in rabbit RBCs, and also caused the shedding of particular membrane proteins.10 Similar effects showing changes in membrane permeability have been reported for human RBCs.11 Some, but not all, studies show a loss of hemoglobin from RBCs irradiated with cell phone frequency microwaves, indicating greater membrane fragility.12 However, these are in vitro studies in which blood taken from the body was directly exposed to microwaves.
The observation that peripheral blood taken from a finger and toe of the same subject showed the same blood changes in response to cell phone radiation exposure suggests that the blood changes we observed are systemic. This deserves further study to investigate whether the observed blood changes are consistent throughout the human body.
The blood effects observed in this study could not conclusively be correlated with the percentage WAPF diet that subjects consumed. Thus, it appears that the WAPF diet did not have a substantial protective effect. However, the percentage WAPF diet was self-reported by subjects and is somewhat unreliable. This study was an initial small exploratory study and did not compare the WAPF diet to other diets in a controlled trial. Thus, we cannot draw firm conclusions on the role of diet.
We did not investigate how long these blood changes last after the cell phone radiation exposure period ends. However, because subjects refrained from using a cell phone for four hours prior to the study, we can surmise that the blood recovers within four hours. The onset, reversibility, recovery time, and chronicity of these blood changes need further investigation.
It is probable that the blood changes we observed would affect blood circulation. RBC aggregation has been widely studied and its importance is well-established in the microcirculation. RBCs that are stuck together in rouleaux or other aggregates increase the blood viscosity, and this affects the passage of RBC through the microvessels throughout the body.13 RBC shape and deformability are also relevant to blood flow. The typical round disk shape of normal RBCs is considered optimum for blood flow. The shape of the echinocytes might impair blood flow and oxygen release from echinocytes is known to be impaired.14 It would be important to explore whether symptoms such as fatigue and poor concentration, characteristic of EHS, may possibly result from the blood changes that we observed in this study.
It is not known whether repeated or chronic exposure to cell phone radiation produces similar effects on the blood as observed in this study. However, we found that older subjects who reportedly use cell phones less in daily life than younger subjects showed greater levels of blood changes. It is possible that younger subjects may simply have greater resilience to cell phone radiation than older subjects. It is also possible that because younger subjects receive more regular exposure, they have become habituated, i.e., less sensitive to it. Their reactivity is diminished, and they may be unable to respond to it appropriately as a stressor due to various long-term changes in their bodies from repeated exposure. Further studies comparing different groups of users by age and cell phone habit could resolve these issues.
Limitations and Delimitations
This is a small short-term study with ten subjects tested in single experimental sessions. Neither experimenter blinding nor control groups were used. However, it was a preliminary study designed to look for any acute effects on the blood. Apparently it is among the first studies of its kind to document visual effects on peripheral blood following short-term human exposure to cell phone radiation. It achieved its goal. Larger, controlled studies should be conducted to expand on these results.
In support of this study, certain controls were used. Subject fasting, exposure to cell phone radiation, and exposure to ambient electrosmog from the local environment were controlled. An unbiased method of selecting and photographing the blood specimens near the sample center to avoid edge effects was used. The researcher has many years of experience in blood microphotography and developed a Likert scale to score blood factors reliably using a well-trained eye. The blood changes recorded by microphotography are objective and visually compelling.
Radiation Protection and Future Prospects
How can we protect ourselves from cell phone radiation? Various commercial devices are being sold with claims of protection. However, controlled trials on these products are lacking. They need testing by independent laboratories and publications in peer-reviewed journals to establish their validity. The method used in this study could be adapted to test such devices for a protective effect on the blood.
The exposure of over 80 percent of the world’s population to cell phone radiation makes this a potentially immense problem that needs more public health champions to raise awareness and educate people. Many users wear microwave transmitters attached to their heads, or carry cell phones in pockets or on hips. These devices remain active, even when turned off, still communicating with the nearest cell phone tower. Pregnant women, and of course children, are believed to be the most vulnerable to cell phone radiation, the latter due to their thinner skulls, developing brains and other organs.15 Yet half of the children in the U.S. as well as many children around the world use cell phones regularly.
In light of these findings and those from other studies on the biological effects of cell phone frequency microwaves, the evidence suggests that their safety is uncertain. Meanwhile people may choose to reduce their exposure to cell phones by changing their habits and usage. The public should demand more independent testing—outside of the industry. More funding should be made available to clarify the nonthermal biological effects of cell phone radiation and to investigate long-term effects, too. This would help establish appropriate safety standards with a solid scientific basis.
The authors of this study wish to keep their names and affiliations confidential.
This study was funded in part by the Weston A. Price Foundation.
Copyright Weston A. Price Foundation, 2015
Notes
1. Pew Research Internet Project, Mobile Technology Fact Sheet, January, 2014. http://www.pewinternet.org/fact-sheets/mobile-technology-fact-sheet/
2. FCC Consumer Guide SAR, Specific Absorption Rate For Cell Phones: What it Means for You. March 12, 2014.http://www.fcc.gov/guides/specific-absorption-rate-sar-cell-phones-what-it-means-you
3. Belyaev I. Non-thermal biological effects of microwaves. Microwave Review, November, 2005, 13-29.
4. Behari J. Biological responses of mobile phone frequency exposure. Indian Journal of Experimental Biology, 2010, 48, 959-981.
5. World Health Organization (WHO), IARC Classifies Radiofrequency electromagnetic fields as possibly carcinogenic to humans. Press Release, May 31, 2011. http://www.iarc.fr/en/media-centre/pr/2011/pdfs/pr208_E.pdf
6. Rubik B. Pilot research study: live blood analysis of adults comparing the Weston A. Price Foundation diet and the conventional modern diet. Wise Traditions in Food, Farming, and the Healing Arts, 2009, 10(4), 35-43.
7. Rubik B. How does pork prepared in various ways affect the blood? Wise Traditions in Food, Farming, and the Healing Arts, 2011, 12(3), 24-32.
8. Brecher G and Bessis M. Present status of spiculed RBCs and their relationship to the discocyteechinocyte transformation, a critical review. Blood 1972, 40 333-344.
9. Alghamdi MS and El-Ghazaly NA. Effects of exposure to electromagnetic fields on some hematological parameters in mice. Open Journal of Medicinal Chemistry, 2012, 2, 30-42.
10. Liburdy RP and Penn A. Microwaves bioeffects in the erythrocyte are temperature and pO2 dependent: cation permeability and protein shedding occur at the membrane phase transition. Bioelectromagnetics 1984, 5(2), 283-291.
11. Savopol T, Moraru R, Dinu A, Kovacs E, Sajin G. Membrane damage of human red blood cells induced by low-power microwave radiation. Electromagnetic Biology 1995, 14, 99-105.
12. Kouzmanova M, Atanasova G, Atanasov N, Tasheva S. Effects of in vitro exposure to GSM900 electromagnetic field on human erythrocytes. Environmentalist, 2007, 27, 423-428.
13. Mchedlishvili G, Varazashvili M, Gobejishvili L. Local RBC aggregates disturbing blood fluidity and causing stasis in microvessels. Clinical Hemorheology and Microcirculation, 2002, 2, 99-106.
14. Reinhart WH and Chien S. Red cell rheology in stomatocyte-echinocyte transformation: roles of geometry and cell shape. Blood, 1986, 67(4), 1110.
15. O’Neill K, Teo C, Davis D, et al. Mobile Phone Health Risks: The Case for Action to Protect Children.www.mobilewise.org, 2011.