

Kunihiko Iida wants the world to know that the atomic bombs the United States dropped on Hiroshima and Nagasaki 75 years ago next month are still claiming lives and causing suffering.
Iida was 3 years old in August 1945. His father had died in battle; he was living with his mother and her parents in a house 900 meters from Hiroshima’s hypocenter, the spot right beneath the detonation. The blast crumpled the house. The family fled the city, but Iida’s mother and older sister soon died from their injuries, a fact the little boy didn’t grasp. “Until I entered elementary school, I thought they were living and that we would meet someday,” he says.
His injuries left him bedridden for years, and he has suffered debilitating illnesses ever since. Childhood anemia caused him to collapse at school. He’s had ulcers and asthma, underwent two surgeries to remove brain tumors, and now has thyroid growths. “There has never been a break in these illnesses,” he says.
Yet Iida has survived. Thousands of others died prematurely over the years because of radiation-induced cancer, a tally that is still growing. Collectively, they have left an important legacy. Most of what is known today about the long-term health effects of radiation has come out of research with those survivors. The work, now run by the Radiation Effects Research Foundation (RERF), is making “major contributions to our understanding of radiation effects,” even today, says Richard Wakeford, a radiation epidemiologist at the University of Manchester. RERF studies also underpin the limits that countries have set for occupational and medical exposure to radiation.
Iida has participated in the studies since the late 1950s, because, he says, “They are trying to accurately grasp the misery of the atomic bomb,” something he hopes will promote peace. People don’t understand the unique impacts of nuclear weapons, Iida says. He and other participants “have helped the entire world,” says Ohtsura Niwa, chairman of RERF.
The survivors’ ranks are now rapidly thinning. About 70% of the original 120,000 participants enrolled in RERF’s Life Span Study (LSS) have died; most of those remaining are in their 80s and 90s. “We have an ethical obligation” to follow the cohort through the last surviving member, Niwa says—but at the same time, “We have to expand our mission.”
RERF researchers believe they can continue to gather epidemiological findings from existing life and health histories of the LSS participants, but they are also starting entirely new studies, for example of the molecular mechanisms by which radiation exposure leads to cancer. And biological samples from 30,000 study participants collected over 7 decades await genomic analysis.
One unanswered question is whether an individual’s exposure to radiation can genetically damage their offspring. “No one can say that there is no effect on the second generation,” says Katsuhiro Hirano, a Hiroshima area schoolteacher whose mother was irradiated; he now heads an association of second-generation bomb survivors that is pushing for greater recognition of their health concerns. So far, there’s no evidence that radiation damage can be passed down, but Hirano says survivors’ worries resonate among others exposed to radiation, including victims of nuclear accidents, power plant workers, and uranium miners. “This campaign is not just about ourselves,” he says. “We want to work with radiation victims the world over.”
The Hiroshima bombing on 6 August 1945 killed an estimated 90,000 to 120,000 people, who died either instantaneously or over the following weeks and months from injuries or acute radiation sickness, the result of damage to bone marrow and the intestinal tract. The bomb that leveled Nagasaki 3 days later claimed another 60,000 to 70,000 lives. The estimates are rough because “there were no bodies left to count near the hypocenter: The heat and energy literally vaporized the closest persons. And many bodies were swept out to sea with the tides, after dying burn victims sought relief in Hiroshima’s numerous rivers,” science sociologist Susan Lindee of the University of Pennsylvania wrote in her 1994 book Suffering Made Real: American Science and the Survivors at Hiroshima.
Within 6 weeks of the bombings, three U.S. and two Japanese expert teams were at work in both cities to study the biological impact of the radiation. Their objectives differed. The Japanese were primarily trying to understand the medical effects on survivors. The Americans wanted to know how and why people died from atomic blast radiation. That might help triage victims—separating those who might be saved from those doomed to die—during future nuclear wars.
The first U.S. teams gathered what information they could and left Japan within months. But in November 1946, U.S. President Harry Truman approved the creation of a broader research effort. Under the umbrella of the National Research Council, a new Atomic Bomb Casualty Commission (ABCC)—RERF’s predecessor—would seize the “unique opportunity for the study of the medical and biological effects of radiation,” Lindee writes, quoting a U.S. Navy proposal. The results would be useful not only during war, but also for peaceful uses of atomic energy. ABCC grew quickly. By 1951, it employed 143 allied and 920 Japanese personnel in Hiroshima and Nagasaki.
One of ABCC’s most immediate concerns was the possible impact of radiation on survivors’ children. It was clear that the bombings affected children already conceived in August 1945, resulting in an increased number of babies born with a small head size. And fruit fly studies showing that irradiation of adults causes heritable genetic changes and birth defects in offspring suggested there might be longer term effects.
To watch for birth defects among children born in later years, ABCC enrolled expecting mothers and had staffers collect information on how close to the hypocentre they and their husbands had been and details on previous pregnancies. After the women gave birth, they recorded any defects and every baby’s sex, weight, length, and head circumference.
The results were “reassuring,” Wakeford says. In a 1953 Science paper, ABCC researchers reported that among more than 60,000 pregnancies between 1948 and 1952, they did not find any correlation between parental exposure and the frequency of malformations and stillbirths or differences in birth weight. They did see hints that irradiation of mothers may have resulted in the birth of more girls whereas fathers’ exposure tended to increase the number of baby boys.
The Japanese public was not convinced. A-bomb survivors, hibakusha in Japanese, have long suffered discrimination over fears they might be physically or psychologically impaired and that their children might inherit genetic defects. The stigma has affected female survivors more than men.
One of them is Michiko Kodama, who was 7 years old and inside a wooden school on the outskirts of Hiroshima on the day of the bombing. She escaped without major injuries, but in the following weeks she lost many relatives to acute radiation sickness, including a beloved cousin who died in her arms, begging for water she couldn’t swallow. Kodama had difficulty finding a job when she finished school, until a teacher helped her land a position at a local company. There, in her early 20s, she met a man who took her to meet his family. His mother told Kodama there was no problem with her background and character. “But you can’t marry my son because you are a hibakusha,” Kodama recalls the woman saying. “People said hibakusha had the blood of the devil.”
Several years later, a friend introduced Kodama to a man who looked past her status. They married and had two daughters. But the bias persists: Years later, the mother of one daughter’s boyfriend opposed their marriage because of the girl’s hibakusha background. The son defied his mother and the young couple married.
The good news about birth defects was counterbalanced in the early 1950s by discouraging findings on another front. “Leukemia is a very rare disease, but clinicians became aware that it was appearing a lot among the survivors,” says Kotaro Ozasa, an RERF epidemiologist. ABCC showed the disease was especially prevalent among those closest to the hypocenter. Previous studies among people exposed to radiation in a medical context had hinted at the link, Wakeford says, but “the findings from Japan provided convincing evidence.”
By then, ABCC was planning to follow the survivors for decades more. A 1950 census had helped identify 280,000 hibakusha all over Japan. From among those still living in Hiroshima and Nagasaki, ABCC recruited about 75,000 for its LSS, along with 25,000 unexposed controls. The cohort covered men and women of all ages, who had been at various distances from the explosions. “That census from 1950 created the entire foundation” of ABCC’s cohorts, says RERF epidemiologist Eric Grant, although another 20,000 people were added later.
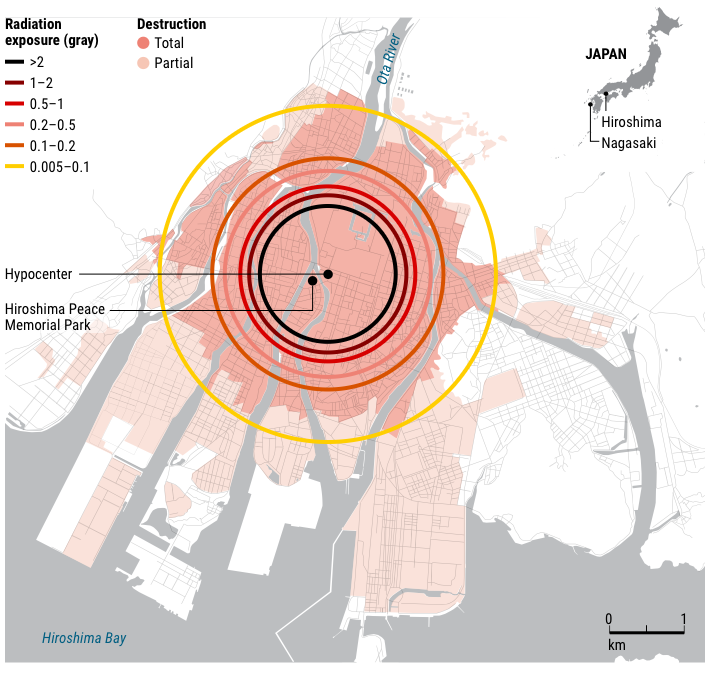
How radiation exposure affected health
Studies in Hiroshima (shown on map below) and Nagasaki conducted over the past 75 years have yielded important insights into the health effects of radiation. Researchers went to great lengths to determine survivors’ exposure, which depended partly on their distance from the hypocenter of the bombings.

Estimating the combined gamma and neutron radiation exposure for each individual was a challenge. Scientists began by calculating the expected radiation at various distances from the hypocenter, then verified those numbers in several ways. They cut samples from the copper roof ornaments of temples, for instance, and used mass spectrometry to check for a nickel isotope created by the bombs’ neutron bombardment. To study the degree to which buildings might have shielded victims, Oak Ridge National Laboratory built several typical Japanese houses at the Nevada Test Site and measured radiation levels inside and outside during atomic bomb tests in 1957 and 1958.
In the 1960s, ABCC also interviewed 28,000 survivors, asking for details on their exact location at the time of the blast, what sort of building they were in and on what floor, and even which way they were facing and whether they had been sitting or standing. The investigators used those details to assign a dose for every person in the LSS. (In the 1980s, they refined their work down to the level of individual organs.)
Year after year, the researchers have tracked the incidence of more than a dozen different types of cancers in the survivors, along with mortality. “Radiation risk is very complex,” says RERF epidemiologist Alina Brenner. It depends on sex and age at exposure and can be influenced by genetic susceptibility and lifestyle factors such as smoking. And risks “change over time as a population ages,” she says. But the sheer size and duration of the LSS, along with its detailed data on exposure, age, and sex, allowed researchers to draw many conclusions as the decades passed.
Dose was clearly very important. Among those who were within about 900 meters of the hypocenter and received more than 2 grays of radiation, 124 have died of cancer. (That dose is about 1000 times the average annual radiation dose from natural, medical, and occupational sources combined.) In its latest LSS update, RERF scientists conclude—based on comparisons of cancer deaths between the exposed group and unexposed controls—that radiation was responsible for 70 of those deaths (see graphic, above). Scientists call this number, 56.5%, the attributable fraction. The numbers of deaths are low because few who were close to ground zero survived the blast, explains Dale Preston, a biostatistician at Hirosoft International who previously worked at RERF. But among these people, “Most of the cancers are due to the radiation,” Preston says.
At 1 gray of exposure, the dose roughly 1100 meters from the hypocenter, the attributable fraction is 34.8%, and it decreases linearly for lower doses. Women suffered more radiation-associated cancers than men, largely because of cases of breast cancer. Both men and women exposed at a younger age were more at risk as they aged: “It’s thought that actively dividing cells are more susceptible to radiation effects, so younger people are more sensitive,” Ozasa says. Radiation most increased the risk of leukemia among survivors, followed by cancer of the stomach, lung, liver, and breast. There was little impact on cancers of the rectum, prostate, and kidney. Exposure also heightened the risk of heart failure and stroke, asthma, bronchitis, and gastrointestinal conditions, but less so; for those with a 2-gray exposure, 16% of noncancer deaths were deemed attributable to radiation.
The findings have had an “outsized influence” on policies and practices to make the use of ionizing radiation safer, says Kimberly Applegate, a radiation health expert retired from the University of Kentucky and a member of the International Commission on Radiological Protection (ICRP). The shielded rooms now routine for x-ray procedures and the dosimetry badges that track the accumulated exposure of health care and nuclear power plant workers are based in part on RERF data. ICRP is also using the data to develop recommendations for space tourists and astronauts traveling to Mars.
Whether RERF’s findings—based on one-time exposure—can shed light on the risks for those exposed to low doses over long periods of time is still a topic of debate. “Nobody really knows” what happens at low doses, says Robert Ullrich, RERF’s head of research. But so far, RERF’s conclusions are consistent with studies of those exposed to low doses at work, he says.
Participants themselves didn’t reap benefits from the studies, at least at first. Many joined expecting treatment for their ills, Iida says. But ABCC did not offer treatment because it might be seen as an admission of responsibility for their suffering by the United States. “ABCC did not have a good reputation among the hibakusha,” Iida says. Its top positions were held by U.S. scientists, adding to strains that led to a reorganization of ABCC into RERF in 1975. Japan and the United States now have equal representation on the Board of Councilors, key positions are split, and both countries contribute roughly half of its annual budget, now $31 million.
RERF now shares tests results and other individual data with study participants and provides them with counseling and referrals; the Japanese government subsidizes health care for most hibakusha. In 2017, at a ceremony marking the 70th anniversary of the commission’s founding, Niwa expressed regret that ABCC had studied bombing victims without treating them. “Survivors still feel there is an asymmetrical relationship” with RERF, says Akiko Naono, a sociologist at Kyoto University who studies hibakusha issues. They are the source of data but still see little in return.
![]()
U.S. researchers studying Hiroshima and Nagasaki bombing victims in 1945 initially worked from train cars. The research continues to this day. (RADIATION EFFECTS RESEARCH ORGANIZATION)
New data are still coming in. In papers published in 2018 and 2019, for example, RERF scientists reported that women exposed to bomb radiation at the age of menarche, the first occurrence of menstruation, were at a higher risk of developing breast or uterine cancer later in life than those exposed before or after puberty. The proliferation of breast and uterine tissue during puberty provides “a lot of potential for DNA damage induced by radiation,” Brenner says.
The breast cancer study also gives a glimpse of RERF’s future agenda. The first analysis did not try to distinguish among the several major breast cancer subtypes, which vary in their biological mechanisms and prognoses, Brenner says. RERF is now analyzing cancerous tissue collected from patients to determine whether any of those subtypes occur more frequently in radiation victims. If so, that could provide hints about just how radiation damages tissue and raises cancer risk.
Samples are one resources RERF has in abundance. During detailed biennial health examinations of more than 23,000 of the survivors (including some exposed in utero), researchers have collected and preserved blood and urine samples, some dating back to the late 1950s. RERF has also amassed frozen cell lines from parents and children in 500 families in which at least one parent was exposed to radiation, plus an equal number of control families.
DNA in those samples—which so far has not been sequenced—could provide a check on the early data about the health of survivors’ offspring. Despite the reassuring findings about birth defects, some researchers worry radiation may have caused mutations in testes and ovaries that children born years later might have inherited. Researchers plan to compare the number and types of mutations found in the families to see whether any are more common in children of radiation-exposed parents, Ullrich says.
RERF hasn’t yet seen any evidence of radiation-linked health effects in a study of 77,000 children of survivors. That could be “because we may not have the statistical power to be able to see” an impact, Ullrich says. Based on the findings, the Japanese government has refused to provide health care or screenings to the second generation.
But the possibility of harm still haunts survivors’ children, including Hirano. His mother, then 20, went searching for relatives in Hiroshima 2 days after the bombing, exposing herself to residual radiation. Hirano has no medical problems, but like many children of survivors, he has stories about health issues in his family. His mother had two stillbirths before he was born, and a cousin, also a second-generation survivor, died of leukemia in his 30s. “Many second-generation A-bomb survivors have great anxiety about their health,” he says. And those directly exposed to the bomb are often wracked with guilt if their children get sick or die, he says. Kodama is an example. Her youngest daughter died of ear canal cancer at age 45 in 2011. Ever since, she has wondered: “Was it because of the damage to my genes?”
Hirano’s association of survivors’ children is now taking the matter to court, seeking recognition as hibakusha and the health care that goes with it. “But the biggest hope of our movement,” he says, “is that there never again be second-generation victims” of atomic bombs.
*
Note to readers: please click the share buttons above or below. Forward this article to your email lists. Crosspost on your blog site, internet forums. etc.
Dennis Normile is a contributing correspondent in Shanghai, China.